| OCR Text |
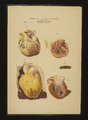
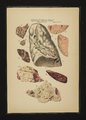
Show 111s11:.\s1<:s or 'ruic onoxxs or Siicriox lll.. T.\111,1-: 1].. Fig.1. lll‘lSl'lltA'l‘lON. [Sicc'rlox lll. seemed. also. not to have been involved in this present pneumonia. A section of the superior and inferior lobes of the lung of the same patient. It shows a whitish. creamy color. and is profusely spread all over with brownish and yellowish white spots (granules). The vesicles show a number of granules. which are made up of blood corpuscles. both red and white. inclosed within a net-work of line and coarse libres. "These libres Jill up the vesicular cavity. and are attached to its walls. and communicate with the interalveolar connective tissue." (_77/1-cr'7'c/1/cris le/Is‘ of pull/o/cy/col I/I's-lo/ot/Iq.) Between some of the lobules the connective tissue was so soft as to readily allow the lob- ules to separate. and showed that some of them were atfected and some were not. The whole inferior lobe showed granite-like line markings. and an intermixture of red and cream-cob)red spots (like some species of marble). 111 the apex of the left lung 21 number of small cavities (cavernau) freely communicat'ed with the bronchi ("121.111111 close to it a These few scattered obsolete tubercles were found. were evidently of long standing. and had nothing to do with the present atfection. The cavities seemed to have been partly contracted by adhesive cicatrizatiou. and tion of the lung are turgid. with blood, They are dilated and the capillaries very tortuous and project far into th 1 alveolar cavities, and thereby partly Ocelude them. The exudation and the extravasation begin by an intiltration of a rich, albuminous, sticky liquid into the tissues. in the septa and the interlobular pleural structure points of 1‘-xtravasated blood are The stagnant blood in the altered capillaries alriady visible. permit great quantities of plasma to ooze out through the wall; the power of absorption is for a time perfectly destroyed ; the Colorless corpuscles along the wall leave the vessels, and the red corpuscles follow soon. This introduces the second stage. The quantity of exudation corresponds with the intensity of the intlannnation. In intense inflammation. when the circulation in the capillaries has completely ceased, and the current in the veins is hemmed, the hypera‘mia drives so 111111-11 more exudate into the tissue the stronger the forward movement of the arterial blood is toward the :apillaries. With the succeeding separation of the colored and colorless corpuscles, the 11p]'1roaching and cohesion ot' these to the vascular wall, the increased hyperaania intensities this stage and enormous exudative masses enter the tissues. In a less intense con- dition, the hyperiemia being less, the alteration of the vascular wall less, the exudation lighter and the stagnation of the blood in the capillaries easier overcome, the second stage is also very much mitigated, and the following phases pass almost unnoticed. To the naked eve such a lung is remarkable for its red color (differing in intensity from the brightest scarlet to the deepest brownisl1-re1l). Its elasticity is nearly gone; it is tough, dense and heavier than a lung tilled with air. \Vhat little air is still existing in the, cells ,‘2111 be readily moved backward and forward, it cannot pass the int'undibular aperture" for it is occluded by a glutinous substance, which prevents the ingress and egress of air. l)yspn1ea is caused by it: equally so the vesicular crepitation. Of course. the lung has temporarily lost the power of respiration. As the patient has as yet not become used to vicariatc the healthy lung for the diseased, he will now sutt‘er much more from dyspn1ea than afterward. The lung in Table I, Fig. l, in this section especially presents the tirst and second stages of an intense case of cronpose pneu- monia. The highly swollen, or rather bloated. appearance of the whole organ, the clear detinition of the interlolnilar spaces. the inttamed, injected. and vascularixed pleura show that a port1o11 of the lung l1as already reached the second stage. (We 111111 in tne same lung, frequently, several stages of the intlammaton, showing this progressive movement of the intlannnation from one portion to the other. of the organ). (‘l1aractcristic of the second stage is the enormously injected pleural covering on the lung, on the basal surface. facing the diaphragnr For the 111ec11anieal friction, which that muscle exerts upon the surface of the lung naturally causes an increase of circulation in that part of it: and in any inttamed condition it will be found that the hyperaemia there. is greater than in less mechanically irritated portions of the organ. [111151]:p1ztl'srtt/oa#111 consequence of the alteration ofthe blood vessels and the stratilication of the blood within them. the free surfaces of the cavities of the air cells become covered with enormous quantities of fibrous exudate. At the same time there is an abundant exuration ot' the colorless. and some colored. cor- All form a complex mass of coarse and line tibrous puseles. threads, which extend from septum 1o septum, through the 11111111- N. 11-11.. 1;. on the tables indicate the bronchial glands. which were here very turgid and tilled with blood clots. 11. bronchi. .\.\'.1\' l'. pulmonary arteries and veins. L. l'. pulmonic lobule). Figures 2 and It show portions of a lung in the sec- ond stage of cronpose inllammation. [hemorrhagic iiilil- tratiou to an extent to completely obliterate all traces of structure. 11 forms a uniform mass of brick-red tissue. with only here and there the whitish or yellowish out- lines of mucus membrane of the bronchi. which have undergone a complete change. from the anaimic con- dition existing in the circulation of their tissue proper. Thcse spots resemble. in their appearance. the diph- theritic patches of the larynx and trachea. They are. likely, of the same nature. and seem 1111c to the same cause. Fig. 1 shows a portion of a lung ("of a young man who died of pneumonia). The apex of the right lung had swiftly become compressed by serous etl'usion. and the structures had become 1edomatous and soft, showing only here and there distinct traces of the pulmonic tissue. dibular and alveolar cavities, and thus till them all with the plastic substance. Of course. the air is nearly all driven out of the cells. and the blood in the capillaries. the small veinlets and arterioles. are only motionless clots. "llere and there some vascular cavities are still open. and the circulation in the lung is preserved in a. vicarious manner. by increased pressure. resulting from the stagnant condition of the blood in the occluded vessels." (1,. lac/11llt‘IlI/I. [)1'1,' .\'lo‘1'1(n_1/1‘n 111‘s Lung/1'11/.‘/'1'/s/1111fs, ['o‘m 1;.7.) .\ hardened section of a portion ot' hepatised lung in this stage shows that the vesicular wall is perfectly undisturbed, In the cellular cavity will be seen a tiuely tibred coagulum. containing large quantities of colorless, and colored corpusclcs, derived from the dilated vessels, The quantity ot' corpuscular elements, especially the colored, in the eoagulum determines the gravity of this stage, and as a general rule, also. the probable termination of the disease-proccss, When the quantity of red corpuscles is very great, and amounting to severe cxtravasation, the result is commonly very unfavorable to the for not only does such a condition indicate a deep patient: vascular disturbance, which does not readily recovcr, but also the blood, as a very easily decomposable substance, will become an additional source of danger to the weakened lung, by inducing secondary disturbances by its decay, etc. These colored blood globules stamp this stage with the name indicated above. The expectorate, if any exists at all. is dark lu'ownish-red 1' rusty spit/11 ). The, color proper to :1 portion of it a lung in this stage is that of an ox liver, when exposed to the air soon after the death of the animal. 11 may vary in color, from an intense blood-red to a deep collee~brown, with reddish specks here and there. The color is not due to the contents of the vessels, but to that of the tissue of the lung. For the quantity of blood in the capillaries diminishes in inverse ratio to the quantity of exudate. The red hepatiscd tissue becomes heavy and dense. .\ cut surface will present a vast 1111111ber of knotty projections of a tolcrably consistent nature. They were once considered to be granulations, but they are really the tibrinous clots lly gently pressing a cut in the alv'eola and int'undibula. portion of a. lung. soon after its removal from the body, these, eoagula, or rather tibrinous cylinders, may be pressed out, and will be found, under the microscope, to be casts of the liner bronchi and int'undibula. ltemak was the lirst to correctly interpret their nature, and described them already in 1813: "The bronchial coagula form branched cylinders, dichotomosly divided. the branches being of lesser diameter than the trunk. The main trunk is generally liner than the lirst einl11‘1111cl1111ents, and ends at its free extremity in line threads. \icry frequently, at the ends of the branehlets, a 111 some of the . widened portion is found.etc. 1111-111 tloat on make which knottv ends air globules are found, and cylinders The clot.) alveolar the by enclosed (An water: bottom, the to sink but tloat, globules containing no air, do not are white, and \Yllciltltescclots:11'1'\\'11sln-1l\\‘itli111111-11 water. they and there llere tibrin. have all the characteristics of washed them llefound surface." their upon found bloodarc some spotsot' pneumonia. 111 in consumptive lungs. and in cases of croupose much crouposc pneumonia of old people, these cylindcrs contain tissue. and are black or brown pigment. derived from the lung thrown out with the sputa. r Through this leather~like parcnchyma. the inspiratoiy murmu the into air of e entranc the at. as form same the in is continued |