A collection of videos relating to the diagnosis and treatment of eye movement disorders. This collection includes many demonstrations of examination techniques.
Dan Gold, D.O., Associate Professor of Neurology, Ophthalmology, Neurosurgery, Otolaryngology - Head & Neck Surgery, Emergency Medicine, and Medicine, The Johns Hopkins School of Medicine.
A collection of videos relating to the diagnosis and treatment of eye movement disorders.
NOVEL: https://novel.utah.edu/
TO
Filters: Collection: "ehsl_novel_gold"
| Title | Description | Type | ||
|---|---|---|---|---|
| 176 |
 |
Leukemic Leptomeningeal Carcinomatosis Causing 4th and 6th Nerve Palsies | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 55-yo-man with CML that recurred as AML. Diagonal diplopia developed, and on examination he was found to have a partial right 6th nerve palsy, in addition to a left hypertropia that increased in right gaze, down... | Image/MovingImage |
| 177 |
 |
Li Maneuver for Geotropic Right HC-BPPV, Canalithiasis | The Li maneuver is used to treat horizontal canal, canalithiasis. When compared to the Gufoni maneuver, the Li maneuver was as effective to treat HC-BPPV and there was no significant difference between the maneuvers; however, the Li Maneuver may take less time to complete. 1. The patient starts in a... | Text |
| 178 |
 |
Li Maneuver for Geotropic Right HC-BPPV, Canalithiasis (Video) | The Li maneuver is used to treat horizontal canal, canalithiasis. When compared to the Gufoni maneuver, the Li maneuver was as effective to treat HC-BPPV and there was no significant difference between the maneuvers; however, the Li Maneuver may take less time to complete. 1. The patient starts in a... | Image/MovingImage |
| 179 |
 |
Liberatory or Modified Semont, Posterior Canal Benign Paroxysmal Positional Vertigo (BPPV) for Right Posterior Canal BPPV (Canalithiasis or Cupulolithiasis) | Posterior canal (PC) accounts for 70-90% cases of BPPV [1-3] and resolves with canalith repositioning maneuvers 90% of the time [4-13]. The Semont/Liberatory maneuver is considered a gold-standard treatment, with class 1 evidence for use and success rates close to 90% [4-13].The Liberatory maneuver ... | Text |
| 180 |
 |
Liberatory or Modified Semont, Posterior Canal Benign Paroxysmal Positional Vertigo (BPPV) for Right Posterior Canal BPPV (Canalithiasis or Cupulolithiasis) | Posterior canal (PC) accounts for 70-90% cases of BPPV [1-3] and resolves with canalith repositioning maneuvers 90% of the time [4-13]. The Semont/Liberatory maneuver is considered a gold-standard treatment, with class 1 evidence for use and success rates close to 90% [4-13].The Liberatory maneuver ... | Image/MovingImage |
| 181 |
 |
Light Near Dissociation in a Tonic Pupil | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 65-year-old woman who noticed difficulty reading and heightened sensitivity to lights OS for the last 6 months. On examination, there was mydriasis OS of about 6 mm (3 mm OD). The left (mydriatic) pupil constric... | Image/MovingImage |
| 182 |
 |
Localization of Ophthalmoplegia | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: A table describing the localization of ophthalmoplegia. | Text |
| 183 |
 |
Maddox Rod and Red Glass Testing | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: Describing the basics of strabismus. | Text |
| 184 |
 |
Measuring Divergence Amplitude | Divergence insufficiency should be suspected in patients with binocular horizontal diplopia at distance (but not near) who lack abduction deficits. There should be an esodeviation greater at distance, and in older patients with levator dehiscence (or previous ptosis surgery) and prominent superior s... | Image/MovingImage |
| 185 |
 |
Medial Longitudinal Fasciculus Syndrome with Prominent Spontaneous Nystagmus | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 60-year-old man who experienced the abrupt onset of diplopia and imbalance. He had typical features of a left medial longitudinal fasciculus (MLF) syndrome including left internuclear ophthalmoplegia (INO) and l... | Image/MovingImage |
| 186 |
 |
Medial Medullary Syndromes | This is a video of two patients who suffered small strokes involving the right medial medulla, and who presented with acute vertigo and oscillopsia. The first patient in the video had pure upbeat nystagmus, while the second patient had upbeat-torsional (towards the right ear) nystagmus in addition t... | Image/MovingImage |
| 187 |
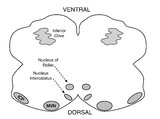 |
Medullary Structures Relevant to Upbeat Nystagmus | This is an axial section of the medulla, slightly more caudal as compared to (please refer to figure "medullary structures relevant to the ocular motor and vestibular consequences of the lateral medullary (Wallenberg) syndrome). Again seen are the inferior cerebellar peduncle (ICP) and caudal aspect... | Image |
| 188 |
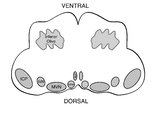 |
Medullary Structures Relevant to the Ocular Motor and Vestibular Consequences of Lateral Medullary (Wallenberg) Syndrome | This is an axial section of the medulla showing the structures that, when damaged, are responsible for the vestibular and ocular motor features of the lateral medullary or Wallenberg syndrome. The nucleus prepositus hypoglossi (NPH) and medial vestibular nucleus (MVN) complex is important for horizo... | Image |
| 189 |
 |
Mesodiencephalic Stroke Causing Unilateral riMLF and INC Ocular Motor Syndromes | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 65-year-old man who experienced the sudden onset of diplopia (with horizontal and vertical components), dysarthria and imbalance. An MRI performed the following day showed a left mesodiencephalic stroke. The pat... | Image/MovingImage |
| 190 |
 |
Mild 6th Nerve Palsy Due to Pontine Stroke | This is a 70-year-old woman with HTN and diabetes who presented with horizontal diplopia for several weeks, worse in right gaze. There was a very subtle abduction paresis OD with full motility elsewhere. With cover-uncover testing, there was a small esotropia in right gaze (esodeviation seen with al... | Image/MovingImage |
| 191 |
 |
Miller Fisher Syndrome - Ophthalmoplegia and Hyperreflexia | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 45-yo-woman who presented with mild imbalance and diplopia. There had been a preceding viral illness several weeks prior. Examination demonstrated horizontal gaze paresis (sparing unilateral adduction), mild gai... | Image/MovingImage |
| 192 |
 |
Miller Fisher Syndrome - Ophthalmoplegia, Ptosis and Ataxia | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a young man who presented with ptosis, difficulty moving the eyes and gait imbalance several weeks after a GI illness. Miller Fisher syndrome was diagnosed, IVIG therapy was initiated, and anti-Gq1b antibodies cam... | Image/MovingImage |
| 193 |
 |
Modified (Chair) Dix-Hallpike | The safety of the patient should be prioritized when completing this test virtually, and the examiner should avoid putting the patient in a position where a fall may occur. Modified (chair) Dix-Hallpike:(1) this test can be used for patients who may not be able to safely undertake the traditional Di... | Image/MovingImage |
| 194 |
 |
Modified Zuma for Right Horizontal Canal Canalithiasis (Geotropic Nystagmus) | The Modified Zuma maneuver is used to treat horizontal canal canalithiasis (geotropic nystagmus. 1. Patient begins in a seated position. 2. The patient's head is rotated 45 degrees towards the unaffected side. 3. The patient transitions to lying on their affected side and maintains this position for... | Text |
| 195 |
 |
Modified Zuma for Right Horizontal Canal Canalithiasis (Geotropic Nystagmus) (Video) | The Modified Zuma maneuver is used to treat horizontal canal canalithiasis (geotropic nystagmus. 1. Patient begins in a seated position. 2. The patient's head is rotated 45 degrees towards the unaffected side. 3. The patient transitions to lying on their affected side and maintains this position for... | Image/MovingImage |
| 196 |
 |
Monocular Downbeat Nystagmus Due to a Posterior Fossa Cyst | This is a 40-yo-man who experienced months of imbalance and was found to have an epidermoid cyst (immediately posterior to the 4th ventricle), which was resected. Months after surgery, he experienced monocular vertical oscillopsia. On examination, there was subtle downbeat nystagmus (DBN) in the rig... | Image/MovingImage |
| 197 |
 |
Monocular Horizontal Pendular Nystagmus in MS | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: Both of these patients have MS and monocular (OS) horizontal pendular nystagmus. The first patient seen in the video has normal afferent function and no evidence of optic nerve disease in either eye, while the second pati... | Image/MovingImage |
| 198 |
 |
Multiple Cranial Neuropathies Due to Glomus Tumor | This is a woman who was diagnosed with a right sided glomus tumor, and subsequently underwent resection. Seen here are multiple cranial neuropathies related to the tumor itself as well as to the surgery. She cannot abduct the right eye due to a right CN VI palsy. She has a right lower motor neuron f... | Image/MovingImage |
| 199 |
 |
Multiple Lower Cranial Neuropathies Following Carotid Endarterectomy | This is a patient who underwent a right carotid endarterectomy (CEA). Following the surgery, multiple right sided lower cranial nerves were involved. In his case, there was trapezius and sternocleidomastoid weakness and atrophy on the right, indicative of right CN XI injury. There was an absent gag ... | Image/MovingImage |
| 200 |
 |
Neuro-Ophthalmic Features and Pseudo-MG Lid Signs in Miller Fisher Syndrome | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 51-year-old woman who presented with imbalance, acute onset dizziness and diplopia that developed over three days following two weeks of upper respiratory infection and bacterial conjunctivitis. When she was ini... | Image/MovingImage |