A collection of videos relating to the diagnosis and treatment of eye movement disorders. This collection includes many demonstrations of examination techniques.
Dan Gold, D.O., Associate Professor of Neurology, Ophthalmology, Neurosurgery, Otolaryngology - Head & Neck Surgery, Emergency Medicine, and Medicine, The Johns Hopkins School of Medicine.
A collection of videos relating to the diagnosis and treatment of eye movement disorders.
NOVEL: https://novel.utah.edu/
TO
| Title | Description | Type | ||
|---|---|---|---|---|
| 226 |
 |
Horner's Syndrome with Anhidrosis | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a patient with the onset of ptosis OD years prior, with clear evidence of a Horner's syndrome. Imaging of the oculosympathetic tract was unrevealing. The patient also mentioned that with exercise, the left side of... | Image/MovingImage |
| 227 |
 |
Skew Deviation and the Triad of the Ocular Tilt Reaction (OTR) | This is a patient who presented with vertical diplopia, who was found to have a complete ocular tilt reaction including the following features: (1) Skew deviation - right hypertropia that was about 30 prism diopters in all directions of gaze including right, left, up, down, as well as in right and ... | Image/MovingImage |
| 228 |
 |
Mesodiencephalic Stroke Causing Unilateral riMLF and INC Ocular Motor Syndromes | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 65-year-old man who experienced the sudden onset of diplopia (with horizontal and vertical components), dysarthria and imbalance. An MRI performed the following day showed a left mesodiencephalic stroke. The pat... | Image/MovingImage |
| 229 |
 |
Medial Longitudinal Fasciculus Syndrome with Prominent Spontaneous Nystagmus | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 60-year-old man who experienced the abrupt onset of diplopia and imbalance. He had typical features of a left medial longitudinal fasciculus (MLF) syndrome including left internuclear ophthalmoplegia (INO) and l... | Image/MovingImage |
| 230 |
 |
Paroxysmal Ocular Tilt Reaction | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 60-year-old woman who 2 years prior experienced a left sided hypertensive hemorrhagic stroke, resulting in right hemiparesis, dysarthria and vertical diplopia. The initial vertical diplopia resolved completely a... | Image/MovingImage |
| 231 |
 |
Alternating Hypertropias - Bilateral 4th Nerve Palsies and Alternating Skew Deviation | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: Seen here are two patients with alternating hypertropias. The first is a 70-year-old woman with a diagnosis of cerebellar ataxia, neuropathy, vestibular areflexia syndrome (CANVAS). In the video, both spontaneous downbeat... | Image/MovingImage |
| 232 |
 |
Isolated Central 4th Nerve Palsy | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 40-year-old man with a right hypertropia that worsened in left and down gaze in addition to right head tilt, and improved in left head tilt. There was subjective excyclotorsion OD with double Maddox rod testing.... | Image/MovingImage |
| 233 |
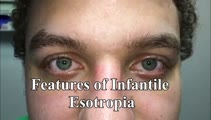 |
Eye Signs in Infantile Esotropia - Latent Nystagmus and Inferior Oblique Overaction | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 25-yo-man with a history of amblyopia and intermittent eye crossing. On exam, he had a comitant 25 prism diopter esotropia, and other features of infantile (or congenital) esotropia including: latent nystagmus (... | Image/MovingImage |
| 234 |
|
PSP with Complete Ophthalmoplegia and Inability to Suppress the VOR | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 65-year-old woman presenting with visual complaints in the setting of advanced progressive supranuclear palsy (PSP). She had complete vertical and horizontal ophthalmoplegia, although the vestibulo-ocular reflex... | Image/MovingImage |
| 235 |
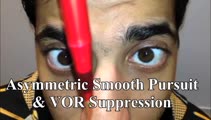 |
Saccadic Smooth Pursuit and Vestibulo-ocular Reflex Suppression (VORS) | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 20-yo-man who suffered a left MCA stroke years prior. Upon evaluation of his eye movements, saccades and all classes of eye movements were normal, although his smooth pursuit and VORS were choppy to the left (ip... | Image/MovingImage |
| 236 |
 |
Head-Shaking (2-3 Hz) | Head-shaking: instruct the patient to close their eyes and perform active rapid head-shaking at 2-3 Hz for ~15 secs. If a unilateral vestibulopathy is present, head-shaking-induced (contralesional) nystagmus is often provoked, with the slow phase toward the affected ear. With central lesions, the ny... | Image/MovingImage |
| 237 |
 |
Typical Features of Duane Syndrome Type 1 | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a patient seen for vestibular complaints, who on exam, was found to have (unrelated to her vestibular symptoms) impaired abduction OS. In adduction, there was narrowing of the palpebral fissure OS, a result of glo... | Image/MovingImage |
| 238 |
 |
Duane's Syndrome Type III | This is a 40-yo-woman seen in neurology clinic for a complaint unrelated to her eyes. On exam, there was impaired adduction and abduction OS. In adduction, there was narrowing of the palpebral fissure OS, a result of her globe retraction due to co-contraction of the medial and lateral rectus muscles... | Image/MovingImage |
| 239 |
 |
Convergence | Can bring out or change the direction of vertical nystagmus in Wernicke's, or cerebellar disease; may be impaired in Parkinson's disease, head trauma, elderly patients; may overcome an adduction deficit with an INO. Instructional ocular motor examination procedures. | Image/MovingImage |
| 240 |
 |
Gaze-Evoked and Centripetal Nystagmus in Creutzfeldt-Jakob Disease | This is a 65-year-old woman who experienced a progressive cerebellopathy over several months. Initially, she presented with mild gait imbalance and positional vertigo, and there was only apogeotropic positional nystagmus (more pronounced in supine roll test compared to Dix-Hallpike) with a very slig... | Image/MovingImage |
| 241 |
|
Test Your Knowledge: The Acute Vestibular Syndrome with Gaze-Evoked Nystagmus and Bilaterally Abnormal Head Impulse Testing Due to Middle Cerebellar Peduncle and Flocculus Hemorrhage | This is a 70-year-old woman with a history of atrial fibrillation on warfarin presenting with acute prolonged vertigo and imbalance. In addition to the findings demonstrated in the first part of the video, what else should be seen to reassure the examiner that the etiology of her vertigo is benign? ... | Image/MovingImage |
| 242 |
|
Test Your Knowledge - Central and Peripheral Vestibular and Ocular Motor Signs Due to a Large Vestibular Schwannoma | Which of the following is least likely to be the correct localization or etiology given the findings seen in the video? 1) Acute right 8th cranial neuropathy 2) Right-sided vestibular schwannoma 3) Right vestibular nucleus infarction 4) Right anterior inferior cerebellar artery distribution stroke A... | Image/MovingImage |
| 243 |
 |
Downbeat Nystagmus and Cerebellar Atrophy | This is a 40-year-old man with 2 years of progressive ataxia and oscillopsia. On examination, he had downbeat nystagmus (DBN), an ocular motor finding that is usually (but not always) associated with flocculus/paraflocculus dysfunction, which causes overaction of the anterior canal (upward or anti-g... | Image/MovingImage |
| 244 |
|
Test Your Knowledge - Vertical Saccadic Palsy Due to Bilateral riMLF Infarctions | This is a 30-year-old who was found minimally responsive on the lounge floor of an ice skating rink. He was brought to the ED, where he had a GCS score of 8 (where 15 is normal) for poor responsiveness. His ocular motor exam is shown in the video. Regarding Finding #1, which of the following is fals... | Image/MovingImage |
| 245 |
|
Square Wave Jerks and Macrosaccadic Oscillations in a Patient with a Cerebellar Tumor | This is a 40-year-old man who developed severe headaches, confusion, and gait imbalance which led to neuroimaging which demonstrated a midline cerebellar mass with compression of the fourth ventricle and obstructive hydrocephalus. He underwent a suboccipital craniectomy for resection of the mass, an... | Image/MovingImage |
| 246 |
 |
Ocular Dipping and Ping-pong Gaze Due to Bi-hemispheric Strokes | This is a 51-year-old man presenting with hypertensive left thalamic intracerebral hemorrhage and intraventricular hemorrhage, with course complicated by multifocal supratentorial ischemic strokes. He developed abnormal movements characterized by slow, conjugate, horizontal deviations, consistent wi... | Image/MovingImage |
| 247 |
 |
Apraclonidine Testing in Horner's syndrome | This patient experienced relatively abrupt ptosis and was seen and diagnosed with a Horner's syndrome within a few days of the onset. There were no other exam findings and history did not offer clues as to the etiology. Neuroimaging of the oculosympathetic tract was unrevealing. Apraclonidine testin... | Image/MovingImage |
| 248 |
 |
Range of Motion (Ductions) | Range of motion (ductions): check the range of each individual eye (ductions) if there is diplopia or if a motility deficit is suspected. Instructing the patient to hold their head 20o to the right or to the left may provide a better view of the range of horizontal gaze, if there is diplopia or if a... | Image/MovingImage |
| 249 |
 |
Smooth Pursuit | Smooth pursuit: instruct the patient to hold their head steady, fix their eyes on the camera and slowly move the camera in the horizontal and vertical planes. Or, have the patient focus on their outstretched thumbnail (or other small fixation target), while following the slowly moving object horizon... | Image/MovingImage |
| 250 |
 |
Slow Horizontal, Vertical, Oblique Saccades and Gaze-evoked Nystagmus in Anti-AGNA-1 Encephalitis | This is a patient who presented subacutely with imbalance and dizziness. On examination, she had evidence of gaze evoked nystagmus, right internuclear ophthalmoplegia, as well as slow saccades horizontally and vertically. She was diagnosed with a rare antibody-mediated disorder, anti-AGNA-1 (antig... | Image/MovingImage |