A collection of videos relating to the diagnosis and treatment of eye movement disorders. This collection includes many demonstrations of examination techniques.
Dan Gold, D.O., Associate Professor of Neurology, Ophthalmology, Neurosurgery, Otolaryngology - Head & Neck Surgery, Emergency Medicine, and Medicine, The Johns Hopkins School of Medicine.
A collection of videos relating to the diagnosis and treatment of eye movement disorders.
NOVEL: https://novel.utah.edu/
TO
| Title | Description | Type | ||
|---|---|---|---|---|
| 1 |
 |
+ HIT, + Skew, Unidirectional Nystagmus: Central Acute Vestibular Syndrome Due to Wallenberg Syndrome | This is a 45-year-old woman who presented to the ED with acute prolonged vertigo and vertical diplopia. She was seen as an outpatient 1 month after her ED visit, and double vision and balance were improving by that time. Her HINTS testing showed the following (seen in the video): 1) Head Impulse - A... | Image/MovingImage |
| 2 |
 |
3rd Nerve Palsy With Preserved 4th Nerve Function | 80-yo-woman with a left vasculopathic 3rd nerve palsy (minimal pupil involvement of about 1 mm relative mydriasis OS - other etiologies ruled out and resolved as expected over months). Although the inferior rectus is paretic, intact superior oblique muscle function can be demonstrated by asking the ... | Image/MovingImage |
| 3 |
 |
6th Nerve Palsy as Initial Presentation of Metastatic Lung Cancer | A video describing 6th nerve palsy as initial presentation of metastatic lung cancer. | Image/MovingImage |
| 4 |
 |
A 'Canal Jam' During Head Impulse Testing in a Patient With Horizontal Canal BPPV | A 70-year-old man reported brief episodes of positional vertigo. Ten years prior, he had undergone gamma knife radiosurgery for a vestibular schwannoma at the left cerebellopontine angle. Video head impulse testing (vHIT) showed reduced gains and corrective saccades in the planes of the left horizon... | Image/MovingImage |
| 5 |
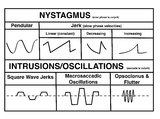 |
A Comparison of Nystagmus and Saccadic Intrusions/Oscillations | Nystagmus can be classified into pendular and jerk waveforms, where both are generated by a slow, pathologic phase. Corrective phase (the position reset mechanism) differs. In pendular nystagmus, the eyes move back and forth with about the same velocity and amplitude, similar to that of a pendulum... | Image |
| 6 |
 |
A flowchart approach to nystagmus/intrusions | In tandem with the flowchart, the following added clues should be used to help with etiology: i) vector [horizontal, vertical, torsional]; ii) binocular or monocular; iii) spontaneous or provoked [e.g., BPPV]; iv) change with monocular viewing or gaze direction; v) rest of history, neurologic, and o... | Image/StillImage |
| 7 |
 |
Aberrant Regeneration of the 3rd Nerve | Aberrant regeneration in two patients: 1) a young woman with a right cavernous sinus meningioma with subsequent development of aberrant regeneration demonstrated by eyelid elevation OD in attempted downgaze (i.e., some fibers that were supposed to innervate the right IR were misrouted to the right l... | Image/MovingImage |
| 8 |
 |
Abnormal Active Head Impulse Testing Recorded Asynchronously in Bilateral Vestibular Loss | This is a video of patient with the subacute onset of head movement-dependent oscillopsia due to bilateral vestibular loss (with obvious bilaterally abnormal head impulse test (HIT) at the bedside), in addition to central ocular motor signs including saccadic smooth pursuit and gaze-evoked nystagmus... | Image/MovingImage |
| 9 |
 |
Abnormal Head Impulse Test in Vestibular Neuritis 1 Week After Onset | This is a 25-year-old woman who experienced the acute vestibular syndrome due to right-sided vestibular neuritis 1 week prior to this video. Left-beating nystagmus (LBN) was only noted in left gaze, but with fixation-removed, there was clear LBN in primary position that increased with head-shaking a... | Image/MovingImage |
| 10 |
 |
Abnormal Visually-Enhanced VOR in Cerebellar Ataxia, Neuropathy, Vestibular Areflexia Syndrome (CANVAS) | A 67 year old woman presented with 1 year of progressive numbness, gait instability, and oscillopsia when walking or with head movements. Examination showed excessive square-wave jerks, bilateral horizontal gaze-evoked nystagmus, impairment of the visually-enhanced vestibular ocular reflex (vVOR - s... | Image/MovingImage |
| 11 |
 |
Acquired Elliptical Pendular Nystagmus Suppressed by Blinks and Saccades | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 70-year-old man who experienced the gradual onset of oscillopsia over weeks about 3 months prior to this video recording. Examination demonstrated elliptical pendular nystagmus which was atypical for infantile n... | Image/MovingImage |
| 12 |
 |
Active Head Impulse Test | Active head impulse test (HIT): instruct the patient to fix their eyes on the camera and turn their head 20o to the right/left, and then make a rapid movement toward the midline to align their head with the camera again, keeping their eyes fixed on the camera throughout. A simple instruction is to a... | Image/MovingImage |
| 13 |
|
Acute Vestibular Neuritis With Unidirectional Nystagmus and Abnormal Video Head Impulse Test | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is 45-year-old man who presented to the emergency department (ED) 2 days prior to this video recording with acute onset prolonged vertigo, nausea, head motion intolerance, unsteadiness and spontaneous nystagmus, cons... | Image/MovingImage |
| 14 |
 |
The Acute Vestibular Syndrome in MS Due to Middle Cerebellar Peduncle/Root Entry Zone Lesion | This is a 13 year-old girl with relatively abrupt onset vertigo and oscillopsia. On exam, there was primarily right-beating nystagmus in primary gaze with a slight upward (upbeat) component, giving the nystagmus an oblique appearance. The upward component and lack of a clear torsional component acut... | Image/MovingImage |
| 15 |
 |
The Acute Vestibular Syndrome with Dysarthria, Dysphagia, Dysphonia, Hemi-ataxia, and Saccadic Dysmetria Due to the Lateral Medullary (Wallenberg) Syndrome | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 50-year-old woman with the acute onset of vertigo, dysarthria, dysphagia and dysphonia/hoarseness (nucleus ambiguus), ptosis and imbalance. Her examination localized to a left lateral medullary (Wallenberg) synd... | Image/MovingImage |
| 16 |
 |
Acute Vestibular Syndrome with Ocular Tilt Reaction Due to Bacterial Labyrinthitis | This is a patient who initially presented with the acute vestibular syndrome (AVS, e.g., acute prolonged vertigo, spontaneous nystagmus) and right sided hearing loss, and was diagnosed with bacterial labyrinthritis. Her HINTS (Head Impulse, Nystagmus, Test of Skew) testing indicated a central etiolo... | Image/MovingImage |
| 17 |
 |
Acute Vestibular Syndrome With Skew Deviation and Positive Head Impulse Test Due to a Demyelinating Lesion | This is a patient who initially presented with the acute vestibular syndrome (AVS, e.g., acute prolonged vertigo, spontaneous nystagmus). ; See https://collections.lib.utah.edu/details?id=187730 for additional history. ; Her HINTS (Head Impulse, Nystagmus, Test of Skew) testing indicated a central e... | Image/MovingImage |
| 18 |
 |
The Acute Vestibular Syndrome with Skew Deviation, Gaze-evoked Nystagmus, and Bilaterally Abnormal Head Impulse Testing Due to AICA Stroke | This is a 60-year-old man with the acute onset of prolonged vertigo and nystagmus, consistent with the acute vestibular syndrome (AVS). HINTS (Head Impulse, Nystagmus, Test of Skew) exam demonstrated a central pattern: 1) Head impulse test (HIT) was abnormal to the right and to the left. An abnormal... | Image/MovingImage |
| 19 |
 |
The Affected-Ear-up 90 degree Maneuver (HC-Canalithiasis) | The Affected-Ear-up 90 degree Maneuver is used to treat horizontal canal-canalithaisis. 1. The patient starts in a supine position. 2. The patient rotates their head 90 degrees towards the unaffected side. 3. The patient sits up. | Text |
| 20 |
 |
The Affected-Ear-up 90 degree Maneuver (HC-Canalithiasis) (Video) | The Affected-Ear-up 90 degree Maneuver is used to treat horizontal canal-canalithaisis. 1. The patient starts in a supine position. 2. The patient rotates their head 90 degrees towards the unaffected side. 3. The patient sits up. | Image/MovingImage |
| 21 |
|
Alternating Hypertropias - Bilateral 4th Nerve Palsies and Alternating Skew Deviation | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: Seen here are two patients with alternating hypertropias. The first is a 70-year-old woman with a diagnosis of cerebellar ataxia, neuropathy, vestibular areflexia syndrome (CANVAS). In the video, both spontaneous downbeat... | Image/MovingImage |
| 22 |
 |
An Approach to the Patient with (Recent Onset) Spontaneous Episodic Vestibular Syndrome | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: A vascular etiology should always be on the differential diagnosis of the recent onset of the spontaneous (unprovoked) episodic vestibular syndrome (EVS), especially in the older population and when vascular risk factors ... | Image |
| 23 |
 |
An Approach to the Patient with Acute Onset Prolonged Vertigo | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: A vascular etiology should always be on the differential diagnosis of the acute onset prolonged vertigo, especially in the older population and when vascular risk factors are present. However, young patients can suffer fr... | Image |
| 24 |
 |
Anterior Canal - BPPV: Deep Head Hanging | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: Regardless or whether it is thought that the patient has right or left anterior canal (AC) involvement, the deep head hanging maneuver is performed in the same way. • First the patient is placed in the long-sitting posi... | Image/MovingImage |
| 25 |
 |
Anterior Canal BPPV | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: Although the anterior canal (AC) variant of benign paroxysmal positional vertigo (BPPV) is rare, mainly owing to its orientation relative to gravity (which makes otoconial debris much less likely to enter it), it can occu... | Image/MovingImage |
| 26 |
 |
Anti-GAD Associated Cerebellopathy and Bilateral Vestibulopathy | This is a 70-year-old woman with the subacute onset of severe imbalance and dizziness. On her initial examination, she had prominent gaze-evoked nystagmus and bilateral vestibular loss. Smooth pursuit was saccadic, although her vestibulo-ocular reflex (VOR) suppression was much smoother. Usually pur... | Image/MovingImage |
| 27 |
 |
Apogeotropic and Downbeat Central Positional Nystagmus Provoked While Seated | This is a young man with intermittent complaints of positional vertigo. With Dix-Hallpike and roll testing, he had apogeotropic positional nystagmus (e.g., right beating nystagmus with the left ear down, and left beating nystagmus with the right ear down) in addition to strong downbeat nystagmus in... | Image/MovingImage |
| 28 |
 |
The Apogeotropic Variant of Horizontal Canal BPPV | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a patient with the apogeotropic (nystagmus beating towards the sky) variant of right horizontal canal (HC) benign paroxysmal positional vertigo (BPPV). In a patient with geotropic (nystagmus beating towards the gr... | Image/MovingImage |
| 29 |
 |
Approach to the Ocular Motor and Vestibular History and Examination | History and examination of ocular motor and vestibular. | Text |
| 30 |
 |
Assessing for Hyperventilation-induced Nystagmus | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: Hyperventilation induced nystagmus is tested by asking the patient to take quick deep breaths (~1/s) for 40-60 seconds. This decreases ICP and increases CSF pH. This can be helpful in diagnosing irritative conditions of ... | Image/MovingImage |
| 31 |
 |
Assessing Utricle Pathway Function and the Effects of Convergence on Nystagmus in Acute Vestibular Neuritis | A 35-year-old woman presented a few days after the onset of room-spinning vertigo. She denied diplopia, dysarthria, dysphagia, dysphonia, incoordination, numbness, and weakness. On examination, she had subtle spontaneous right-beat nystagmus (RBN). This nystagmus increased in amplitude and frequency... | Image/MovingImage |
| 32 |
 |
Atypical Ocular Motor Features (Gaze-evoked Nystagmus) in PSP | This is a 70-yo-woman who met clinical and radiologic diagnostic criteria for progressive supranuclear palsy (PSP). Typical ocular motor features of PSP include square wave jerks, hypometric saccades, choppy pursuit/VORS, impaired down>upgaze (supranuclear in origin) and impaired down>upward saccade... | Image/MovingImage |
| 33 |
 |
Audiometry | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: Audiometry is the measurement of the sensitivity and range of an individual's hearing. As many etiologies of imbalance, nystagmus, vertigo and/or dizziness can have an otologic origin the audiogram is an important piece o... | Text |
| 34 |
 |
Audiometry: What Does It Look Like and How Do I Interpret It? | An audiogram measures a patient's auditory threshold responses with pure-tone stimuli across a range of sound frequencies that are important for human communication, typically 250 Hz to 8000 Hz. The threshold is the sound intensity level at which an individual detects the tone 50% of the time. Heari... | Text |
| 35 |
 |
Basics of Acute Stroke Treatment | A brief overview of management of acute stroke treatment. | Text |
| 36 |
 |
BBQ Roll for Right Horizontal Canal BPPV, Canalithiasis (Geotropic Nystagmus) | The BBQ Roll/Lampert Maneuver has been shown to be an effective treatment and is supported by a level I classification study. 1. The patient starts in a supine position with the head positioned 30 degrees above the horizon. 2. While maintaining head elevation, the patient's head (or whole body) is r... | Text |
| 37 |
 |
BBQ Roll for Right Horizontal Canal BPPV, Canalithiasis (Geotropic Nystagmus) (Video) | The BBQ Roll/Lampert Maneuver has been shown to be an effective treatment and is supported by a level I classification study. 1. The patient starts in a supine position with the head positioned 30 degrees above the horizon. 2. While maintaining head elevation, the patient's head (or whole body) is r... | Image/MovingImage |
| 38 |
 |
The Bedside Examination of the Ocular Motor System | A masterclass covering the bedside examination of the ocular motor system. | Image/MovingImage |
| 39 |
 |
Bilateral 6th Nerve Palsies Due to Idiopathic Intracranial Hypertension | This is a 25-year-old woman who presented with diplopia and blurry vision. On exam, she was found to have papilledema and bilateral 6th nerve palsies. Her opening pressure was >40 cm of water with a normal CSF analysis, and neuroimaging was unremarkable aside from subtle findings that have been asso... | Image/MovingImage |
| 40 |
 |
Bilateral Horizontal Gaze Palsy and Oculopalatal Tremor Due to Pontine Hemorrhage | This 70-yo-woman experienced headache and diplopia and was found to have a hemorrhage centrally within the dorsal pons. Months after the onset, the patient was seen in clinic and had no horizontal eye movements (pursuit, saccades, VOR) in either eye, suggestive of bilateral nuclear 6th nerve palsies... | Image/MovingImage |
| 41 |
 |
Bilateral INOs and Partial 3rd Nerve Palsies | This is a 45-year-old man with progressive ptosis and ophthalmoparesis. 10 years prior to presentation, he experienced diplopia and had a hyperintense lesion involving the medial longitudinal fasciculus (MLF) per report. Over time, he developed bilateral adduction paresis, ptosis and upgaze paresis ... | Image/MovingImage |
| 42 |
|
Bilateral INOs Due to Stroke | This is a 65-year-old man with multiple vascular risk factors who experienced the abrupt onset of diplopia 6 months prior to this video. MRI done within 24 hours of onset was unremarkable. Examination demonstrated subtle bilateral adduction lag with horizontal saccades. There was very mild abducting... | Image/MovingImage |
| 43 |
 |
Bilateral Pseudo-abducens Palsies Due to Midbrain Stroke | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a man who suffered right>left midbrain strokes due to endocarditis complaining of ptosis and inability to move his eyes as well as hallucinations (peduncular hallucinosis). There was a presumed nuclear 3rd nerve p... | Image/MovingImage |
| 44 |
|
Bilateral riMLF Syndrome Causing Vertical Saccadic Palsy and Loss of Ipsitorsional Fast Phases | This is a 60-year-old man who developed fatigue and diabetes insipidus about 12 months prior to this video, and MRI demonstrated hypothalamic enhancement at that time. Nine months prior to this video, he gradually noticed that he was unable to look down. Work-up for ischemic, infectious, inflammator... | Image/MovingImage |
| 45 |
|
Bilateral Vestibular Loss With Gaze-Evoked Nystagmus and Saccadic Visually Enhanced VOR | This is 55-year-old man with the subacute onset of head movement-induced oscillopsia and dizziness. He had a history of psoriatic arthritis. He had not used medications known to be vestibulo-toxic such as gentamicin. ; Salient findings on his examination included 1) bilateral vestibular loss (BVL) d... | Image/MovingImage |
| 46 |
|
Bilaterally Abnormal Head Impulse Test | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This video is an example of bilaterally abnormal head impulse test (HIT) due to bilateral vestibular loss (BVL). Typical symptoms in BVL: head movement-induced dizziness and jumping vision for years with visual jumping/b... | Image/MovingImage |
| 47 |
 |
Bow and Lean Test | The Bow and Lean Test is used to identify the affected side and is designed to be used in conjunction with or after the Supine Roll Test. Within this test a null point may exist where the nystagmus will extinguish because the cupula is in a gravity neutral position. As this test involves the patient... | Text |
| 48 |
 |
Bow and Lean Test (Video) | The Bow and Lean Test is used to identify the affected side and is designed to be used in conjunction with or after the Supine Roll Test. Within this test a null point may exist where the nystagmus will extinguish because the cupula is in a gravity neutral position. As this test involves the patient... | Image/MovingImage |
| 49 |
 |
Brainstem Ocular Motor Machinery | Seen here is a sagittal view of the brainstem. The medulla has a significant role in gaze-holding, and the nucleus prepositus hypoglossi (NPH, along with the medial vestibular nucleus ) is the horizontal neural integrator. The abducens (6th) nucleus is located in the dorsal pons, and sends off the 6... | Image/MovingImage |
| 50 |
 |
Brandt-Daroff Exercises | Brandt-Daroff exercises are less effective than the Epley and the Semont maneuvers and are not shown to prevent recurrence [1-3]. Brandt-Daroff exercises may still be beneficial for habituation exercises and to reduce phobic responses to lying supine or side-lying after the resolution of BPPV. This ... | Text |
| 51 |
 |
Brandt-Daroff Exercises (Video) | Brandt-Daroff exercises are less effective than the Epley and the Semont maneuvers and are not shown to prevent recurrence [1-3]. Brandt-Daroff exercises may still be beneficial for habituation exercises and to reduce phobic responses to lying supine or side-lying after the resolution of BPPV. This ... | Image/MovingImage |
| 52 |
 |
Bruns Nystagmus (During Video-Oculography) Due to Vestibular Schwannoma | A 25-year-old man with a history of right-sided hearing loss, headaches and imbalance was found to have a right vestibular schwannoma on MRI, and underwent a partial resection and radiotherapy. He denied symptoms of head movement dependent oscillopsia (i.e., suggestive of significant unilateral or b... | Image/MovingImage |
| 53 |
 |
Bruns Nystagmus Due to a Cerebellopontine Angle Tumor | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 15-yo-girl who experienced headache and imbalance leading to an MRI which showed a left sided cerebellopontine angle (CPA) tumor. Because of involvement of the left brainstem/cerebellum (e.g., dysfunction of the... | Image/MovingImage |
| 54 |
 |
Caloric Testing | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: Caloric testing is a peripheral vestibular test which takes advantage of the fact that the labyrinth is sensitive to temperature changes. Warm stimulation causes excitation of the semicircular canals while cold stimulatio... | Image/MovingImage |
| 55 |
 |
The Canalith Repositioning Maneuver/Epley Maneuver for Right Posterior Canal Benign Paroxysmal Positional Vertigo | Posterior canal (PC) accounts for 70-90% cases of BPPV [1-3] and resolves with canalith repositioning maneuvers 90% of the time [4-20]. The Epley maneuver is considered a gold-standard treatment, with class 1 evidence for use. | Text |
| 56 |
 |
The Canalith Repositioning Maneuver/Epley Maneuver for Right Posterior Canal Benign Paroxysmal Positional Vertigo (Video) | Posterior canal (PC) accounts for 70-90% cases of BPPV [1-3] and resolves with canalith repositioning maneuvers 90% of the time [4-20]. The Epley maneuver is considered a gold-standard treatment, with class 1 evidence for use. | Image/MovingImage |
| 57 |
 |
Cavernous Sinus Mass Causing Right 3rd and 4th Nerve Palsies | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: 25-yo-man who complained of diplopia and was initially found to have right 4th and 6th nerve palsies in the setting of a right cavernous sinus mass (subsequently diagnosed as Ewing's sarcoma). When seen in follow-up (this... | Image/MovingImage |
| 58 |
 |
Central (Nuclear) 3rd Nerve Palsies | Shown here are two patients with left sided midbrain pathology (hemorrhage and ischemia) which caused damage to the 3rd nucleus. Both of the patients have ipsilateral mydriasis, adduction, supra- and infraduction paresis. Ipsilateral>contralateral ptosis is also present, and localizes to the central... | Image/MovingImage |
| 59 |
 |
Central 4th Nerve Palsy with Contralateral Horner's Syndrome | This is a 60-yo-woman who presented with a complaint of diplopia. Examination demonstrated a left hypertropia that worsened in right and down gaze as well as in left head tilt, and a left 4th nerve palsy was diagnosed. There was also evidence of a mild motility deficit in down/medial gaze OS, consis... | Image/MovingImage |
| 60 |
 |
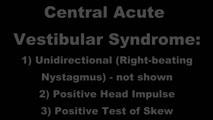
Central Acute Vestibular Syndrome Due to Posterior Fossa Hemorrhage | This is a patient presenting with the acute vestibular syndrome (AVS, e.g., acute prolonged vertigo, spontaneous nystagmus) whose HINTS (Head Impulse, Nystagmus, Test of Skew) testing indicated a central etiology based on negative (normal) head impulse testing (HIT). Nystagmus was unidirectional and... | Image/MovingImage |
| 61 |
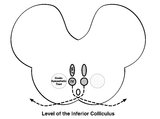 |
Central Anatomy of the Fourth Nerve | The IVth or trochlear nucleus is located ventral to the central periaqueductal grey matter, dorsal to the medial longitudinal fasciculus (MLF) and medial to the oculosympathetic tract at the level of the inferior colliculus. The fascicles of the IVth nerve travel dorsally and caudally around the cen... | Image |
| 62 |
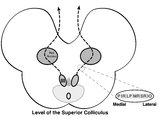 |
Central Anatomy of the Third Nerve | Seen here is an axial section of the midbrain at the level of the superior colliculus. The paired nuclei are located ventral to the periaqueductal grey, and the midline central caudal nucleus (CCN) is located between the right and left nuclei. The CCN sends projections to bilateral levator palpebrae... | Image |
| 63 |
 |
Central HINTS (With an Abnormal Head Impulse Sign) in the Acute Vestibular Syndrome Due to Lateral Pontine/Middle Cerebellar Peduncle Demyelination | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 30-year-old man presenting with vertigo, diplopia and mild left facial weakness (not seen in the video). On exam, there was right-beating nystagmus (RBN) in primary gaze that increased in right gaze (in accordan... | Image/MovingImage |
| 64 |
|
Central Positional Vertigo and Nystagmus in a Posterior Fossa Tumor | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 30-year old woman who presented with positional vertigo and vomiting following a concussion related to a car accident 3 months prior. She was initially diagnosed with posterior canal (PC) benign paroxysmal posit... | Image/MovingImage |
| 65 |
|
Central Vestibular Nystagmus in Anti-DPPX Encephalitis | This is a young woman who presented with oscillopsia due to spontaneous nystagmus in addition to gastrointestinal symptoms which led to the diagnosis of anti-DPP axis encephalitis. She was treated with rituximab, and experience gradual improvement over time. However, years after the onset, she con... | Image/MovingImage |
| 66 |
 |
Centripetal Nystagmus Example | A 68-year-old female reported a 2-year history of progressive gait imbalance, falls, dizziness and vertical oscillopsia. She described that dizziness and oscillopsia were worst when looking down. There was no family history of ataxia. Composite gaze with fixation was recorded with video-oculography ... | Image/MovingImage |
| 67 |
 |
Cerebellar Ataxia, Neuropathy, & Vestibular Areflexia Syndrome (CANVAS): Impaired Visually-Enhanced VOR and Abnormal Head Impulse Testing | A 67 year old woman presented with 1 year of progressive numbness, gait instability, and oscillopsia when walking or with head movements. Examination showed excessive square-wave jerks, bilateral horizontal gaze-evoked nystagmus, impairment of the visually-enhanced vestibular ocular reflex (vVOR - s... | Image/MovingImage |
| 68 |
 |
Cerebellar Degeneration with Downbeat Nystagmus Provoked by Convergence | Description: This is a 70-yo-woman with a progressive gait disorder, diagnosed with cerebellar ataxia. She displayed typical cerebellar ocular motor signs including gaze-evoked nystagmus, choppy pursuit and VOR suppression, and there was very subtle spontaneous downbeat nystagmus, best appreciated w... | Image/MovingImage |
| 69 |
 |
Cerebellar Eye Signs in SCA8 | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 30-yo-man with a diagnosis of SCA 8 who had appendicular and gait ataxia in addition to choppy smooth pursuit and VORS, downbeat nystagmus, saccadic hypermetria, and gaze-evoked nystagmus with rebound nystagmus.... | Image/MovingImage |
| 70 |
 |
Change in Pendular Nystagmus from Oculopalatal Tremor over a Four-year Period | This is a patient who developed oculopalatal tremor months following a pontine hemorrhage. Although it is not shown here, she also has palatal tremor. In the first video which was taken 1 year after her hemorrhage, a vertical-torsional pendular nystagmus can be seen, that is mildly dissociated giv... | Image/MovingImage |
| 71 |
 |
Chiari Malformation Causing Downbeat Nystagmus in Lateral Gaze | This is a 20-yo-man who presented with oscillopsia in lateral gaze from downbeat nystagmus (DBN). In primary gaze, very subtle DBN was only noted with ophthalmoscopy, but in lateral gaze, prominent DBN was present. Other central ocular motor signs included gaze-evoked nystagmus (GEN) vertically, in ... | Image/MovingImage |
| 72 |
|
Chronic Facial Nerve Palsy with Aberrant Regeneration | This is a 35-year-old woman who was diagnosed with right sided Bell's palsy six months prior. Contrast-enhanced MRI at that time was normal. This video demonstrates the phenomenon of aberrant regeneration (synkinesia) of the facial nerve. Due to aberrant regeneration, at rest the right palpebral fi... | Image/MovingImage |
| 73 |
 |
Chronic Progressive External Ophthalmoplegia (CPEO) and Cerebellar Signs | This is a 60-yo-woman who initially presented with imbalance and ophthalmoparesis. Initially, there was mild horizontal gaze limitation with mild gaze-evoked nystagmus and slow saccades, and over the years, gait ataxia and dysarthria (mainly a scanning quality to her speech) developed, and her ophth... | Image/MovingImage |
| 74 |
 |
Common Neuro-Ophthalmic Ancillary Tests to Assist in the Diagnosis and Localization of Afferent Disorders | Chart of the common neuro-ophthalmic ancillary tests to assist in the diagnosis and localization of afferent disorders. | Text |
| 75 |
 |
Complete Microvascular 6th Nerve Palsy with Slow Abducting Saccade | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 90-year-man with HTN, HLD, DM who woke up with horizontal diplopia. Two years prior, he was diagnosed with a microvascular right 6th nerve palsy that resolved over several months. There was little concern for gi... | Image/MovingImage |
| 76 |
 |
Complete Peripheral Vestibulopathy & Ipsilateral Facial Palsy | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: 60-yo-man who suffered the fairly abrupt onset (over hours) of right lower motor neuron facial nerve palsy (7th cranial nerve), vertigo and deafness in the right ear (8th cranial nerve). Vesicles were noted on otoscopy, a... | Image/MovingImage |
| 77 |
|
Complete Saccadic Palsy Due to Pulmonary Thrombectomy | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 37-year-old woman who underwent pulmonary thrombectomy for a pulmonary embolus. Immediately following the procedure, she was unable to make normal eye movements. This video exam (she is the passenger in a car du... | Image/MovingImage |
| 78 |
 |
Congenital Nystagmus | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: Presented here are two patients with congenital nystagmus demonstrating characteristic features including: mixed pendular and jerk nystagmus (usually gaze-evoked) waveforms, stays horizontal even in vertical gaze, suppres... | Image/MovingImage |
| 79 |
 |
Convergence | Convergence: instruct the patient to focus on their thumb held at arm's length, and slowly move their thumb towards their nose. This may bring out or cause reversal of vertical nystagmus (e.g., transition from upbeat to downbeat nystagmus in Wernicke's encephalopathy [see example of transition from ... | Image/MovingImage |
| 80 |
 |
Convergence Insufficiency and Square Wave Jerks in PSP | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 70-yo-woman with progressive supranuclear palsy with complaints of difficulty reading. Her husband noticed that she would frequently close one eye when attempting to read, and words were not clear on the page, a... | Image/MovingImage |
| 81 |
 |
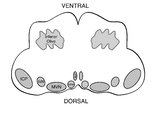
Coronal Section of the Brainstem Showing Ocular Motor Nuclei and Anatomy of the Vestibular Nucleus (with SCC Inputs) | (A) Seen here is a coronal view of the brainstem showing the locations of the ocular motor nuclei (IIIrd, IVth, VIth) as well as the nuclei of VII and VIII (vestibular and cochlear). The vestibular nucleus (VN) is divided into the inferior, lateral, medial, and superior subnuclei, and the medial ves... | Image |
| 82 |
|
Curved Oblique Saccades and Saccadic Slowing in a Patient with an Anti-GAD Mediated Posterior Fossa Syndrome | This is a patient who developed muscle spasms especially involving the muscles of the trunk in addition to a progressive gait disorder. Examination demonstrated slow saccades, slower horizontally than vertically, in addition to gaze evoked nystagmus with a side pocket pattern. Side pocket nystagmu... | Image/MovingImage |
| 83 |
 |
Demonstration of HINTS Examination in a Normal Subject | In the acute vestibular syndrome - consisting of acute prolonged vertigo, spontaneous nystagmus, imbalance, nausea/vomiting, head motion intolerance which is typically due to vestibular neuritis or posterior fossa stroke - a 3 step test of ocular motor and vestibular function known as HINTS, has hig... | Image/MovingImage |
| 84 |
|
Dissociated Elliptical Pendular Nystagmus in MS | This is a patient with multiple sclerosis who presented with oscillopsia. Seen in the video is an elliptical pendular nystagmus in both eyes that was dissociated. Here, the term "dissociated" refers to the fact that the nystagmus is (slightly) more intense in the left eye as compared to the right ... | Image/MovingImage |
| 85 |
 |
Dix-Hallpike | The safety of the patient should be prioritized when completing this test virtually, and the examiner should avoid putting the patient in a position where a fall may occur. Floor (or bed) Dix-Hallpike: this test can be used for patients who are fully mobile and able to get down to the floor and up a... | Image/MovingImage |
| 86 |
 |
Dix-Hallpike Maneuver in Posterior BPPV with Reversal of Nystagmus on Sitting Up | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a patient with typical posterior canal (PC) benign paroxysmal positional vertigo (BPPV), which is provoked by the Dix-Hallpike maneuver. When the patient is moved into the right Dix-Hallpike maneuver, after a brie... | Image/MovingImage |
| 87 |
 |
Downbeat (Perverted) Head Shaking Nystagmus in a Patient with Spontaneous Torsional Nystagmus | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 75-year-old woman with vascular risk factors who experienced abrupt onset imbalance and dizziness. Symptoms were maximal at onset, and she denied progression over 6 months. Clinically, it was felt that she had s... | Image/MovingImage |
| 88 |
 |
Downbeat Nystagmus | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 40-year-old man with 2 years of progressive ataxia and oscillopsia. On examination, he had downbeat nystagmus (DBN), an ocular motor finding that is usually (but not always) associated with flocculus/parafloccul... | Image/MovingImage |
| 89 |
|
Downbeat Nystagmus and Cerebellar Atrophy | This is a 40-year-old man with 2 years of progressive ataxia and oscillopsia. On examination, he had downbeat nystagmus (DBN), an ocular motor finding that is usually (but not always) associated with flocculus/paraflocculus dysfunction, which causes overaction of the anterior canal (upward or anti-g... | Image/MovingImage |
| 90 |
 |
Downbeat Nystagmus and Convergence Spasm | This is a 60-yo-woman with vertical oscillopsia related to her downbeat nystagmus, and diplopia related to an intermittent esotropia. When the esotropia was present, with versions there were bilateral abduction deficits. With ductions and the vestibulo-ocular reflex, it was apparent that the range o... | Image/MovingImage |
| 91 |
|
Downbeat Nystagmus with Active Horizontal Head Shaking | This is a 70-year-old man who presented with one single complaint for 10 years - if he moved his head too quickly (even one single horizontal head movement to the right or the left), he would experience the abrupt loss of balance and dizziness. His typical episodes were reproducible, and interesting... | Image/MovingImage |
| 92 |
 |
Duane's Syndrome Type III | This is a 40-yo-woman seen in neurology clinic for a complaint unrelated to her eyes. On exam, there was impaired adduction and abduction OS. In adduction, there was narrowing of the palpebral fissure OS, a result of her globe retraction due to co-contraction of the medial and lateral rectus muscles... | Image/MovingImage |
| 93 |
 |
Dynamic Visual Acuity | Dynamic Visual Acuity: the examiner can use screen-sharing to provide a visual acuity chart. Instruct the patient to sit at the appropriate distance from their screen at which the lowest line on the visual acuity chart is just readable. Have the patient move their head (horizontally to evaluate the ... | Image/MovingImage |
| 94 |
 |
Dynamic Visual Acuity | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: After assessing static binocular visual acuity, dynamic visual acuity (DVA) is determined by repeating the test during horizontal and vertical head shaking at 2-3 Hz. Dynamic visual acuity is most important to test when ... | Image/MovingImage |
| 95 |
 |
Elliptical Pendular Nystagmus in MS | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 40-yo-woman with MS and bilateral optic nerve disease who presented with a year's long history of oscillopsia, which was related to elliptical pendular nystagmus. The appearance of elliptical nystagmus is the re... | Image/MovingImage |
| 96 |
 |
ENG, VNG, & VOG | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: Electronystagmography (ENG), and videonystagmography (VNG) or videooculography (VOG) are a collection of tests of eye movements that are performed either using surface electrodes around the eye (ENG) or with video goggles... | Text |
| 97 |
 |
Enhanced Ptosis in Myasthenia Gravis | This is a 20-yo-woman who presented with generalized weakness, ptosis and ophthalmoplegia. She had severe ptosis OU at baseline, but when one eyelid was manually elevated, there was marked enhanced ptosis of the opposite eyelid. This was in accordance with Hering's law of equal innervation of the le... | Image/MovingImage |
| 98 |
 |
The Episodic Vestibular Syndrome | This is a 55-year-old man with 6 months of episodic vertigo without clear triggers/provocative factors, with each of his 3 previous episodes lasting less than 5 minutes. While in the clinic, he had one of his typical vertigo attacks. There was initially 30 seconds of right-beating-torsional nystagmu... | Image/MovingImage |
| 99 |
 |
Evaluation of Auditory Function Using Rinne and Weber Tests | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: The Rinne test is an assessment of auditory thresholds to air and bone conduction of sound. The Weber test is a comparison of bone conducted sound of either ear. Conductive hearing loss results in a loss of air conducte... | Image/MovingImage |
| 100 |
 |
Evaluation of Convergence | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: The assessment of convergence includes measuring alignment at near versus distance (see video, https://collections.lib.utah.edu/details?id=187677), near point of convergence and convergence amplitude. Near point of conve... | Image/MovingImage |
| 101 |
 |
Examples of Patients with Saccadic Intrusions (Square Wave Jerks) | Seen here are patients with saccadic intrusions that do have an intersaccadic interval. Square wave jerks are commonly seen in degenerative conditions, mainly involving the posterior fossa (e.g., cerebellar degeneration) and basal ganglia (e.g., progressive supranuclear palsy). | Image/MovingImage |
| 102 |
 |
Expanded Nystagmus & Saccadic Intrusions/Oscillations Differential | Expanded nystagmus & saccadic intrusions/ oscillations differential | Text |
| 103 |
 |
Eye Closure and Oculopalatal Tremor | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This patient suffered a traumatic brain injury with brainstem injury resulting in damage to Mollaret's triangle and palatal tremor. Inferior olivary hypertrophy was noted on her MRI, although no vertical and/or torsional ... | Image/MovingImage |
| 104 |
 |
Eye Handbook App for OKN | Optokinetic nystagmus (OKN): one way this can be examined virtually is using a smartphone application (e.g. Eye Handbook © app used in this video) or optokinetic tape/flag/drum held in front of the examiner's camera. The optokinetic stimulus should occupy the full screen of the patient's device (ea... | Image/MovingImage |
| 105 |
 |
Eyelid Anatomy | Seen here are the major muscles of eyelid opening and closure. The levator palpebrae, which is innervated by the oculomotor nerve, inserts on the tarsus via the levator aponeurosis and directly on the skin of the upper eyelid. The superior tarsal muscle (also known as Muller's muscle, which is inner... | Image |
| 106 |
 |
Eyelid Nystagmus | Lid nystagmus is a rhythmic eyelid movement commonly seen as an epiphenomenon of vertical nystagmus (typically upbeating, as in this case) due to a shared central pathway controlling elevation of the lid and supraduction. There can be isolated lid nystagmus if there is accompanying impairment of su... | Image/MovingImage |
| 107 |
 |
Figure 17: Bony Structures Relevant to the Orbit | The frontal, sphenoid, maxillary, ethmoid, and lacrimal bones make up the orbit. Structures passing through the optic canal include the optic nerve, oculosympathetic tract and ophthalmic artery. Structures passing through the superior orbital fissure include the superior ophthalmic vein, cranial ner... | Image |
| 108 |
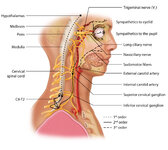 |
Figure 1: Oculosympathetic Pathway for Pupillary Dilation | The oculosympathetic tract is an uncrossed pathway that begins in the hypothalamus, with fibers descending in the brainstem (1st order, commonly affected in a lateral medullary syndrome), synapsing in the lower cervical/upper thoracic spinal cord (interomediolateral cell columns of C8-T2, also refer... | Image |
| 109 |
 |
Figure 24: Typical Visual Field Defects Associated with Discrete Lesions Along the Visual Pathways | Specific monocular or binocular visual field defects can be highly localizing when the neuroanatomy of the visual pathways is understood. The temporal visual field corresponds to the nasal retina, while the nasal visual field corresponds to the temporal retina. 1) Left optic nerve lesion - while an ... | Image |
| 110 |
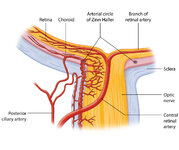 |
Figure 27: Vascular Supply of the Optic Nerve Head, Choroid and Retina | The ophthalmic artery is a branch of the internal carotid artery, which in turn, supplies the posterior ciliary (to choroid and outer retina) and central retinal (to inner retina) arteries. The central retinal artery (CRA) enters the optic nerve about 1 cm posterior to the globe, and an embolus may ... | Image |
| 111 |
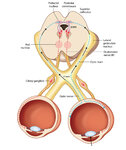 |
Figure 2: Parasympathetic Pathway for Pupillary Constriction | A bright light is shone in one eye, light enters the pupil and hyperpolarizes retinal photoreceptors which activates retinal ganglion cells. These signals propagate along the optic nerves, chiasm, optic tracts, and fibers responsible for the light reflex then synapse in the dorsal midbrain (prior to... | Image |
| 112 |
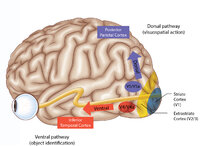 |
Figure 43: How the Brain Makes Sense of What It Sees - The Dorsal and Ventral Visual Pathways, and a 3 Tiered Approach to Vision | 1) Ventral ("what") stream - this begins with the ‘P' retinal ganglion cells à parvocellular layers of the lateral geniculate nucleus (LGN, 3-6) à V1/striate cortex (in blue) à V4/V4a (fusiform and lingual gyri) à occipitotemporal regions. 2) Dorsal ("where") stream - this begins with the ‘M... | Image |
| 113 |
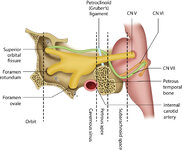 |
Figure 46: The Course of the 6th (VI) Nerve | The sixth nucleus is located dorsally, adjacent to the 4th ventricle, in the lower pons. The genu of the facial (7th) nerve wraps around the 6th nucleus, creating the facial colliculus, which bulges into the 4th ventricle. After the 6th nerve leaves the pons, it follows a vertical course along the c... | Image |
| 114 |
 |
Figure 50: Anatomy and Physiology of the Saccadic Pathways | When a saccade is desired (or reflexively triggered), signals project from the saccade-related cortical eye fields to the superior colliculus, which serves to integrate and relay commands to the saccade generating brainstem circuitry. The inferior cerebellar peduncle (ICP) carries climbing fibers to... | Image |
| 115 |
 |
Figure 51: Lateral Medullary Lesion Causing Saccadic Dysmetria | A lesion of the left lateral medulla and inferior cerebellar peduncle (ICP) will cause decreased climbing fiber inhibition of the left dorsal vermis causing simple-spike (inhibitory) discharge of Purkinje cells to increase. Increased Purkinje cell firing leads to increased inhibition of the ipsilate... | Image |
| 116 |
 |
Figure 53: Vascular Distribution and Anatomy Relevant to the Lateral Medullary (Wallenberg) Syndrome | This axial section of the medulla highlights those structures that, when damaged, are responsible for the vestibular and ocular motor features of the Wallenberg syndrome. The nucleus prepositus hypoglossi (NPH) and medial vestibular nucleus (MVN) complex is important for horizontal gaze-holding (neu... | Image |
| 117 |
 |
Figure 61: Vascular Distribution and Anatomy (Including 6th, 7th, 8th Nerves, MLF) of the Pons | In this axial section of the pons, the proximity of the 7th (VII) and 8th (VIII) fascicles can be appreciated, and a lateral inferior pontine syndrome (anterior inferior cerebellar artery, AICA territory), which could involve both of these fascicles, could cause acute prolonged vertigo accompanied b... | Image |
| 118 |
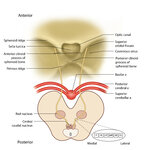 |
Figure 64: The Course of the 3rd (III) Nerve | The 3rd nucleus lies at the ventral border of the periaqueductal gray matter, at the level of the superior colliculus. In between the two nuclei is the midline central caudal nucleus (CCN), which innervates bilateral levator palpebrae muscles (explaining how a unilateral nuclear 3rd can cause bilate... | Image |
| 119 |
 |
Figure 65: Vascular Distribution and Anatomy (Including 3rd Nerve) of the Rostral Midbrain | In this axial section of the midbrain at the level of the superior colliculus, the paired 3rd nuclei are located ventral to the periaqueductal grey, and the midline central caudal nucleus (CCN) is located in between. The fascicles that exit the IIIrd nuclei carry the fibers destined to innervate the... | Image |
| 120 |
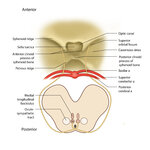 |
Figure 68: The Course of the 4th (IV) Nerve | The 4th nucleus lies at the ventral border of the periaqueductal gray matter, at the level of the inferior colliculus. The fascicles exit the nucleus dorsally and decussate at the anterior medullary velum (anterior floor of the fourth ventricle), and then exit the brainstem dorsally. The peripheral ... | Image |
| 121 |
 |
Figure 69: Vascular Distribution and Anatomy (Including 4th Nerve) of the Caudal Midbrain | In this axial section of the midbrain at the level of the inferior colliculus, the 4th nuclei are located ventral to the periaqueductal grey, dorsal to the medial longitudinal fasciculus (MLF) and medial to the oculosympathetic tract. Fascicles exit the nucleus dorsally and decussate at the anterior... | Image |
| 122 |
 |
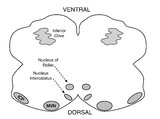
Figure 80: Vascular Distribution and Anatomy Relevant to the Medial Medullary Syndrome | This axial section of the medulla highlights those structures that, when damaged, are often responsible for spontaneous upbeat nystagmus (UBN). The nucleus of Roller and nucleus intercalatus normally have an inhibitory influence over the cerebellar flocculus, and when there is a lesion of Roller/int... | Image |
| 123 |
|
Five Common Ocular Motor Signs in Cerebellar Disorders - Saccadic Hypermetria, Saccadic Pursuit & VOR Suppression, Gaze-evoked & Rebound Nystagmus | (1) Saccadic hypermetria - an overshoot of the visual target (2) Saccadic smooth pursuit - due to impaired pursuit and low gain, saccades are needed to keep up with the visual target. This gives it a ‘choppy' appearance. (3) Saccadic vestibulo-ocular reflex (VOR) suppression - another... | Image/MovingImage |
| 124 |
 |
Fixation and Gaze Holding | Fixation and gaze-holding: assess for nystagmus or saccadic intrusions by observing the eyes in primary position. Then instruct the patient to look in each position of gaze, and to hold that position to assess for gaze-evoked nystagmus. In doing so, motility can also be evaluated with both eyes view... | Image/MovingImage |
| 125 |
 |
The Gans Maneuver for Right Posterior Canal Benign Paroxysmal Positional Vertigo | This maneuver is recommended for individuals with cervical restrictions or precautions, as the maneuver avoids cervical hyperextension and may reduce cervical pain associated with repositioning maneuvers. The Epley maneuver has higher subjective and objective success rates compared to the Gans maneu... | Text |
| 126 |
 |
The Gans Maneuver for Right Posterior Canal Benign Paroxysmal Positional Vertigo (Video) | This maneuver is recommended for individuals with cervical restrictions or precautions, as the maneuver avoids cervical hyperextension and may reduce cervical pain associated with repositioning maneuvers. The Epley maneuver has higher subjective and objective success rates compared to the Gans maneu... | Image/MovingImage |
| 127 |
|
Gaze-Evoked and Centripetal Nystagmus in Creutzfeldt-Jakob Disease | This is a 65-year-old woman who experienced a progressive cerebellopathy over several months. Initially, she presented with mild gait imbalance and positional vertigo, and there was only apogeotropic positional nystagmus (more pronounced in supine roll test compared to Dix-Hallpike) with a very slig... | Image/MovingImage |
| 128 |
 |
Gaze-evoked and Rebound Nystagmus in a Cerebellar Syndrome | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: 30-yo-man with the subacute onset of a cerebellar syndrome. After extensive evaluation and progression, it was thought that this represented an autoimmune process and there was some improvement with immunosuppression. He ... | Image/MovingImage |
| 129 |
|
Gaze-Evoked Nystagmus & Slow Saccades Due to Anti-GAD Antibodies in a Patient with Stiff Person Syndrome | This is a 70-year-old woman with a several year long history of imbalance and stiffness. Exam demonstrated axial and lower extremity stiffness, and ocular motor exam demonstrated gaze-evoked nystagmus (e.g., right-beating in right gaze, left-beating in left gaze, up-beating in up gaze), and mild to ... | Image/MovingImage |
| 130 |
 |
Gaze-Evoked, Rebound, and Centripetal Nystagmus in Cerebellar Degeneration | A 68-year-old female reported a 2-year history of progressive gait imbalance, falls, dizziness and vertical oscillopsia. She described that dizziness and oscillopsia were worst when looking down. There was no family history of ataxia. Composite gaze with fixation was recorded with video-oculography ... | Image/MovingImage |
| 131 |
 |
The Geotropic Variant of Horizontal Canal BPPV | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a patient with the geotropic (nystagmus beating towards the ground) variant of left horizontal canal (HC) benign paroxysmal positional vertigo (BPPV). In a patient with geotropic (nystagmus beating towards the gro... | Image/MovingImage |
| 132 |
 |
Gufoni Maneuver for Left Horizontal Canal BPPV, Canalithiasis (Geotropic Nystagmus) | The Gufoni maneuver may be preferable to the BBQ roll, as the Gufoni maneuver does not require the individual to roll or be in a prone position, making the maneuver more feasible to complete for individuals who are elderly, obese and/or experience immobility. Antecedently, some clinicians remember t... | Text |
| 133 |
 |
Gufoni Maneuver for Left Horizontal Canal BPPV, Canalithiasis (Geotropic Nystagmus) (Video) | The Gufoni maneuver may be preferable to the BBQ roll, as the Gufoni maneuver does not require the individual to roll or be in a prone position, making the maneuver more feasible to complete for individuals who are elderly, obese and/or experience immobility. Antecedently, some clinicians remember t... | Image/MovingImage |
| 134 |
 |
Gufoni Maneuver for Right Horizontal Canal-Cupulolithiasis (Apgeotropic Nystagmus) | The Gufoni Maneuver can be used to treat horizontal canal cupulolithaisis. 1. The patient starts in a seated position. 2. The patient transitions quickly to lying on their affected side. 3. The patient lies on their affected side for two minutes with the head in a neutral position. 4. The patient's ... | Text |
| 135 |
 |
Gufoni Maneuver for Right Horizontal Canal-Cupulolithiasis (Apgeotropic Nystagmus) (Video) | The Gufoni Maneuver can be used to treat horizontal canal cupulolithaisis. 1. The patient starts in a seated position. 2. The patient transitions quickly to lying on their affected side. 3. The patient lies on their affected side for two minutes with the head in a neutral position. 4. The patient's ... | Image/MovingImage |
| 136 |
 |
Head-Shaking (2-3 Hz) | Head-shaking: instruct the patient to close their eyes and perform active rapid head-shaking at 2-3 Hz for ~15 secs. If a unilateral vestibulopathy is present, head-shaking-induced (contralesional) nystagmus is often provoked, with the slow phase toward the affected ear. With central lesions, the ny... | Image/MovingImage |
| 137 |
 |
Head-Shaking Nystagmus - A 'Central' Pattern | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: Evaluating for nystagmus provoked by head-shaking, so-called head-shaking nystagmus (HSN), should be performed in all patients with complaints of dizziness or vertigo, regardless of the chronicity. The maneuver is perform... | Image/MovingImage |
| 138 |
|
Head-Shaking-Induced Nystagmus Following Ramsay Hunt Vestibulopathy | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 50-year-old man who experienced the abrupt onset of imbalance, dizziness and left-sided hearing loss 4 months prior to this examination. He was found to have herpetic vesicles in the left external auditory canal... | Image/MovingImage |
| 139 |
 |
Hemifacial Spasm | This is a 45-year-old man with intermittent left facial twitching and eyelid closure for the last 6 months. With observation, spontaneous left facial spasms were seen involving the orbicularis oculi and oris muscles. With voluntary contraction of left facial muscles, with smiling for instance, there... | Image/MovingImage |
| 140 |
 |
HINTS 'Plus' Patterns in the Acute Vestibular Syndrome Based on Location | HINTS ‘Plus' patterns in the acute vestibular syndrome based on location | Text |
| 141 |
 |
HINTS Exam and Saccadic Dysmetria in Lateral Medullary Stroke | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 50-year-old who experienced the abrupt onset of prolonged vertigo following chiropractic therapy 2 months prior. Initial work-up included an MRI and MR angiogram - MR-diffusion weighted imaging showed an acute l... | Image/MovingImage |
| 142 |
 |
Horizontal Gaze Palsy, Facial Nerve Palsy, and Nystagmus Due to Dorsal Pontine Ischemia | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: Presented here are two patients with horizontal gaze and facial palsies due to stroke. The first patient is a 60-year-old man who presented with double vision and hemiparesis due to a right dorsal pontine ischemic stroke.... | Image/MovingImage |
| 143 |
 |
How to Measure Ocular Alignment Virtually | Ocular alignment: the alternate cover test can be performed by instructing the patient to hold their head steady, fix their eyes on the camera (or a more distant target - the closer the fixation target, the more of an exodeviation the examiner will see), and use their cell phone (or a spoon) to occl... | Image/MovingImage |
| 144 |
 |
Hyperventilation | Hyperventilation: instruct the patient to breathe rapidly in and out of their mouth for 40-60 seconds. Alkalosis and changes in ionized calcium may improve conduction through an affected segment of 8th cranial nerve due to vestibular schwannoma (https://collections.lib.utah.edu/details?id=1213447) o... | Image/MovingImage |
| 145 |
 |
Hyperventilation-Induced Downbeat Nystagmus in a Cerebellar Disorder | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 45-year-old woman with a chronic progressive cerebellopathy of unclear etiology (worsening over at least 10 years) characterized by gait and limb ataxia, gaze-evoked nystagmus, saccadic pursuit and vestibulo-ocu... | Image/MovingImage |
| 146 |
 |
Idiopathic Downbeat Nystagmus Exacerbated with Positional Maneuvers | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 45-yo-woman with vertical oscillopsia for 6+ months, found to have downbeat nystagmus on examination. She mainly complained of dizziness and oscillopsia when laying down. She was found to have a significant exac... | Image/MovingImage |
| 147 |
 |
Idiopathic Downbeat Nystagmus, Decreasing with Convergence | This is a 25-yo-woman who experienced vertically oscillopsia for 1 year, and was found to have downbeat nystagmus. Interestingly, there were no other cerebellar ocular motor signs - e.g., normal saccades, smooth pursuit, VOR suppression, and no gaze-evoked nystagmus, although her (pure) downbeat was... | Image/MovingImage |
| 148 |
 |
Impaired Smooth Pursuit and Other Characteristic Ocular Motor Findings in Middle Cerebellar Peduncle Stroke | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 50-year-old woman who underwent resection of a left-sided acoustic neuroma, and post-operatively, she had vertigo, binocular diplopia, left hemi-ataxia and severe gait ataxia. MR diffusion weighted imaging demon... | Image/MovingImage |
| 149 |
 |
Inferior Oblique Overaction in a Congenital 4th Nerve Palsy | 60-yo-man complaining of intermittent oblique diplopia. There was a left hypertropia that worsened in down gaze, right gaze and in left head tilt. There was a large vertical fusional amplitude in addition to a longstanding rightward head tilt, and on examination there was left inferior oblique overa... | Image/MovingImage |
| 150 |
|
The Influence of Convergence on Downbeat Nystagmus | This is a patient presenting with progressive imbalance and oscillopsia over the course of approximately 1 year. On examination, he had cerebellar ataxia in addition to spontaneous downbeat nystagmus (DBN). His downbeat nystagmus increased in lateral and downgaze, which are characteristic features,... | Image/MovingImage |
| 151 |
 |
Ipsitorsional Quick Phases with Head Tilt in a Normal Subject | This is a demonstration of ocular counterroll, which can be seen when the head is tilted to the right or to the left. For example, when the head is tilted to the right, the top poles of both eyes should rotate toward the left ear to keep the top poles oriented with earth vertical. This is part of ... | Image/MovingImage |
| 152 |
 |
Isolated Central 4th Nerve Palsy | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 40-year-old man with a right hypertropia that worsened in left and down gaze in addition to right head tilt, and improved in left head tilt. There was subjective excyclotorsion OD with double Maddox rod testing.... | Image/MovingImage |
| 153 |
 |
Kim Maneuver for Anterior Canal BPPV | The Kim Maneuver for Anterior Canal can be used to treat individuals with anterior canal BPPV. 1. The patient's head is turned 45 degrees towards the unaffected side. 2. The patient transitions into a supine position with the head hanging 30 degrees below the horizon. 3. After two minutes, the head ... | Text |
| 154 |
 |
Kim Maneuver for Anterior Canal BPPV (Video) | The Kim Maneuver for Anterior Canal can be used to treat individuals with anterior canal BPPV. 1. The patient's head is turned 45 degrees towards the unaffected side. 2. The patient transitions into a supine position with the head hanging 30 degrees below the horizon. 3. After two minutes, the head ... | Image/MovingImage |
| 155 |
 |
The Kim Maneuver for Right Horizontal Cupulolithiasis | The Kim Maneuver is used to treat horizontal canal cupulolithiasis cases where the otoconia may be located on either side of the cupula. 1. The patient begins in a supine position. 2. The patient's head is turned 135 degrees towards the affected side and oscillation is applied to the affected side f... | Text |
| 156 |
 |
The Kim Maneuver for Right Horizontal Cupulolithiasis (Video) | The Kim Maneuver is used to treat horizontal canal cupulolithiasis cases where the otoconia may be located on either side of the cupula. 1. The patient begins in a supine position. 2. The patient's head is turned 135 degrees towards the affected side and oscillation is applied to the affected side f... | Image/MovingImage |
| 157 |
 |
Latent Nystagmus and DVD in Infantile Esotropia | This is a 20-year-old woman with infantile esotropia (s/p strabismus surgery as a child) who demonstrated latent nystagmus and presumed dissociated vertical deviation (DVD) OS, which are commonly seen with infantile esotropia (also inferior oblique overaction and monocular nasotemporal asymmetry to ... | Image/MovingImage |
| 158 |
 |
Leukemic Leptomeningeal Carcinomatosis Causing 4th and 6th Nerve Palsies | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 55-yo-man with CML that recurred as AML. Diagonal diplopia developed, and on examination he was found to have a partial right 6th nerve palsy, in addition to a left hypertropia that increased in right gaze, down... | Image/MovingImage |
| 159 |
 |
Li Maneuver for Geotropic Right HC-BPPV, Canalithiasis | The Li maneuver is used to treat horizontal canal, canalithiasis. When compared to the Gufoni maneuver, the Li maneuver was as effective to treat HC-BPPV and there was no significant difference between the maneuvers; however, the Li Maneuver may take less time to complete. 1. The patient starts in a... | Text |
| 160 |
 |
Li Maneuver for Geotropic Right HC-BPPV, Canalithiasis (Video) | The Li maneuver is used to treat horizontal canal, canalithiasis. When compared to the Gufoni maneuver, the Li maneuver was as effective to treat HC-BPPV and there was no significant difference between the maneuvers; however, the Li Maneuver may take less time to complete. 1. The patient starts in a... | Image/MovingImage |
| 161 |
 |
Liberatory or Modified Semont, Posterior Canal Benign Paroxysmal Positional Vertigo (BPPV) for Right Posterior Canal BPPV (Canalithiasis or Cupulolithiasis) | Posterior canal (PC) accounts for 70-90% cases of BPPV [1-3] and resolves with canalith repositioning maneuvers 90% of the time [4-13]. The Semont/Liberatory maneuver is considered a gold-standard treatment, with class 1 evidence for use and success rates close to 90% [4-13].The Liberatory maneuver ... | Text |
| 162 |
 |
Liberatory or Modified Semont, Posterior Canal Benign Paroxysmal Positional Vertigo (BPPV) for Right Posterior Canal BPPV (Canalithiasis or Cupulolithiasis) | Posterior canal (PC) accounts for 70-90% cases of BPPV [1-3] and resolves with canalith repositioning maneuvers 90% of the time [4-13]. The Semont/Liberatory maneuver is considered a gold-standard treatment, with class 1 evidence for use and success rates close to 90% [4-13].The Liberatory maneuver ... | Image/MovingImage |
| 163 |
|
Light Near Dissociation in a Tonic Pupil | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 65-year-old woman who noticed difficulty reading and heightened sensitivity to lights OS for the last 6 months. On examination, there was mydriasis OS of about 6 mm (3 mm OD). The left (mydriatic) pupil constric... | Image/MovingImage |
| 164 |
 |
Maddox Rod and Red Glass Testing | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: Describing the basics of strabismus. | Text |
| 165 |
 |
Measuring Divergence Amplitude | Divergence insufficiency should be suspected in patients with binocular horizontal diplopia at distance (but not near) who lack abduction deficits. There should be an esodeviation greater at distance, and in older patients with levator dehiscence (or previous ptosis surgery) and prominent superior s... | Image/MovingImage |
| 166 |
 |
Medial Longitudinal Fasciculus Syndrome with Prominent Spontaneous Nystagmus | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 60-year-old man who experienced the abrupt onset of diplopia and imbalance. He had typical features of a left medial longitudinal fasciculus (MLF) syndrome including left internuclear ophthalmoplegia (INO) and l... | Image/MovingImage |
| 167 |
 |
Medial Medullary Syndromes | This is a video of two patients who suffered small strokes involving the right medial medulla, and who presented with acute vertigo and oscillopsia. The first patient in the video had pure upbeat nystagmus, while the second patient had upbeat-torsional (towards the right ear) nystagmus in addition t... | Image/MovingImage |
| 168 |
 |
Medullary Structures Relevant to the Ocular Motor and Vestibular Consequences of Lateral Medullary (Wallenberg) Syndrome | This is an axial section of the medulla showing the structures that, when damaged, are responsible for the vestibular and ocular motor features of the lateral medullary or Wallenberg syndrome. The nucleus prepositus hypoglossi (NPH) and medial vestibular nucleus (MVN) complex is important for horizo... | Image |
| 169 |
 |
Medullary Structures Relevant to Upbeat Nystagmus | This is an axial section of the medulla, slightly more caudal as compared to (please refer to figure "medullary structures relevant to the ocular motor and vestibular consequences of the lateral medullary (Wallenberg) syndrome). Again seen are the inferior cerebellar peduncle (ICP) and caudal aspect... | Image |
| 170 |
 |
Mesodiencephalic Stroke Causing Unilateral riMLF and INC Ocular Motor Syndromes | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 65-year-old man who experienced the sudden onset of diplopia (with horizontal and vertical components), dysarthria and imbalance. An MRI performed the following day showed a left mesodiencephalic stroke. The pat... | Image/MovingImage |
| 171 |
 |
Mild 6th Nerve Palsy Due to Pontine Stroke | This is a 70-year-old woman with HTN and diabetes who presented with horizontal diplopia for several weeks, worse in right gaze. There was a very subtle abduction paresis OD with full motility elsewhere. With cover-uncover testing, there was a small esotropia in right gaze (esodeviation seen with al... | Image/MovingImage |
| 172 |
 |
Miller Fisher Syndrome - Ophthalmoplegia and Hyperreflexia | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 45-yo-woman who presented with mild imbalance and diplopia. There had been a preceding viral illness several weeks prior. Examination demonstrated horizontal gaze paresis (sparing unilateral adduction), mild gai... | Image/MovingImage |
| 173 |
 |
Miller Fisher Syndrome - Ophthalmoplegia, Ptosis and Ataxia | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a young man who presented with ptosis, difficulty moving the eyes and gait imbalance several weeks after a GI illness. Miller Fisher syndrome was diagnosed, IVIG therapy was initiated, and anti-Gq1b antibodies cam... | Image/MovingImage |
| 174 |
 |
Modified (Chair) Dix-Hallpike | The safety of the patient should be prioritized when completing this test virtually, and the examiner should avoid putting the patient in a position where a fall may occur. Modified (chair) Dix-Hallpike:(1) this test can be used for patients who may not be able to safely undertake the traditional Di... | Image/MovingImage |
| 175 |
 |
Modified Zuma for Right Horizontal Canal Canalithiasis (Geotropic Nystagmus) | The Modified Zuma maneuver is used to treat horizontal canal canalithiasis (geotropic nystagmus. 1. Patient begins in a seated position. 2. The patient's head is rotated 45 degrees towards the unaffected side. 3. The patient transitions to lying on their affected side and maintains this position for... | Text |
| 176 |
 |
Modified Zuma for Right Horizontal Canal Canalithiasis (Geotropic Nystagmus) (Video) | The Modified Zuma maneuver is used to treat horizontal canal canalithiasis (geotropic nystagmus. 1. Patient begins in a seated position. 2. The patient's head is rotated 45 degrees towards the unaffected side. 3. The patient transitions to lying on their affected side and maintains this position for... | Image/MovingImage |
| 177 |
 |
Monocular Downbeat Nystagmus Due to a Posterior Fossa Cyst | This is a 40-yo-man who experienced months of imbalance and was found to have an epidermoid cyst (immediately posterior to the 4th ventricle), which was resected. Months after surgery, he experienced monocular vertical oscillopsia. On examination, there was subtle downbeat nystagmus (DBN) in the rig... | Image/MovingImage |
| 178 |
 |
Monocular Horizontal Pendular Nystagmus in MS | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: Both of these patients have MS and monocular (OS) horizontal pendular nystagmus. The first patient seen in the video has normal afferent function and no evidence of optic nerve disease in either eye, while the second pati... | Image/MovingImage |
| 179 |
 |
The Most Common Audiovestibular Laboratory Tests, and the Specific Conditions in Which They May Assist in Making or Supporting the Diagnosis | VN = vestibular neuritis; VM = vestibular migraine; VP = vestibular paroxysmia; vHIT = video head impulse test; VNG = video-nystagmography; ENG = electronystagmography; VOG = video-oculography; VEMPs = vestibular evoked myogenic potentials; SCDS = superior canal dehiscence syndrome; BPPV = benign pa... | Text |
| 180 |
 |
The Most Common Vestibular Conditions Categorized by Timing and Triggers, with Specific Historical Features that Should be Sought for Each (Adapted from Approach to the Ocular Motor and Vestibular History and Examination) | Adapted from https://collections.lib.utah.edu/ark:/87278/s64x9bq1 | Text |
| 181 |
 |
The Most Common Vestibular Conditions Categorized by Timing and Triggers, with Specific Ocular Motor and Vestibular Features that Should be Sought for Each | HINTS+ = Head Impulse, Nystagmus, Test of Skew, ‘Plus' bedside assessment of auditory function; HIT = head impulse test; NP = nerve palsy; BPPV = benign paroxysmal positional vertigo; SCDS = superior canal dehiscence syndrome; BVL = bilateral vestibular loss; PPPD = persistent postural perceptual ... | Text |
| 182 |
 |
Multiple Cranial Neuropathies Due to Glomus Tumor | This is a woman who was diagnosed with a right sided glomus tumor, and subsequently underwent resection. Seen here are multiple cranial neuropathies related to the tumor itself as well as to the surgery. She cannot abduct the right eye due to a right CN VI palsy. She has a right lower motor neuron f... | Image/MovingImage |
| 183 |
 |
Multiple Lower Cranial Neuropathies Following Carotid Endarterectomy | This is a patient who underwent a right carotid endarterectomy (CEA). Following the surgery, multiple right sided lower cranial nerves were involved. In his case, there was trapezius and sternocleidomastoid weakness and atrophy on the right, indicative of right CN XI injury. There was an absent gag ... | Image/MovingImage |
| 184 |
 |
Neuro-Ophthalmic Features and Pseudo-MG Lid Signs in Miller Fisher Syndrome | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 51-year-old woman who presented with imbalance, acute onset dizziness and diplopia that developed over three days following two weeks of upper respiratory infection and bacterial conjunctivitis. When she was ini... | Image/MovingImage |
| 185 |
 |
Neuro-Ophthalmic Features and Pseudo-MG Lid Signs in Miller Fisher Syndrome (Figure 1) | This is a 51-year-old woman who presented with imbalance, acute onset dizziness and diplopia that developed over three days following two weeks of upper respiratory infection and bacterial conjunctivitis. When she was initially seen as an outpatient, nystagmus was noted to the right and left, and a ... | Image |
| 186 |
 |
Nystagmus Due to Paraneoplastic (Anti-Yo) Brainstem and Cerebellar Degeneration | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 40-yo-woman with anti-Yo antibody associated with ovarian cancer. Initial symptoms 2.5 years prior (to this video) included imbalance and dysarthria. She complained of oscillopsia which was due to her upbeat nys... | Image/MovingImage |
| 187 |
 |
Ocular Bobbing Due to Hepatic Encephalopathy | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 55-year-old man presented with hepatic encephalopathy, and found to have ocular bobbing. Head CT did not show any acute changes. Ocular bobbing almost always localizes to the pons, although cerebellar pathology ... | Image/MovingImage |
| 188 |
 |
Ocular Dipping and Ping-pong Gaze Due to Bi-hemispheric Strokes | This is a 51-year-old man presenting with hypertensive left thalamic intracerebral hemorrhage and intraventricular hemorrhage, with course complicated by multifocal supratentorial ischemic strokes. He developed abnormal movements characterized by slow, conjugate, horizontal deviations, consistent wi... | Image/MovingImage |
| 189 |
 |
Ocular Motor & Vestibular Features of the MLF Syndrome | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This 61-year-old woman with HTN and DM presented for evaluation of acute onset diagonal diplopia. Adduction OS was about 60% of normal while medialization OS improved with convergence. In right gaze, dissociated abducti... | Image/MovingImage |
| 190 |
 |
Ocular Motor & Vestibular Features of the MLF Syndrome (Figures 1, 2, and 3) | This 61-year-old woman with HTN and DM presented for evaluation of acute onset diagonal diplopia. Adduction OS was about 60% of normal while medialization OS improved with convergence. In right gaze, dissociated abducting nystagmus was present OD, and there was a clear adduction lag when asking he... | Image |
| 191 |
|
Ocular Motor Signs in Brainstem Demyelinating Disease - Spontaneous Upbeat, Vertical Gaze-Evoked Nystagmus, Slow Saccades, Bilateral Vestibular Loss, INOs | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 25-year-old woman who presented with painful vision loss bilaterally two years prior to this video recording, which was diagnosed as optic neuritis. Months later, she experienced oscillopsia and binocular horizo... | Image/MovingImage |
| 192 |
 |
Ocular Motor Signs in Early Progressive Supranuclear Palsy | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 64-year old man who experienced imbalance and falls (usually backwards) for the last 6 months. He experienced difficulty navigating stairs and had become a messy eater (thought to be in large part due to his ver... | Image/MovingImage |
| 193 |
 |
Ocular Motor Signs in Progressive Supranuclear Palsy (PSP) | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 65-yo-woman complaining of imbalance and double vision. She had significant convergence insufficiency (and would close her right eye with near viewing), providing an explanation for her diplopia. Convergence ins... | Image/MovingImage |
| 194 |
 |
Ocular Motor Signs in SCA 6 | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 45-yo-man who was recently diagnosed with SCA 6. There was no clear spontaneous downbeat nystagmus (DBN) in primary gaze, although DBN could clearly be provoked by convergence. Other ocular motor features includ... | Image/MovingImage |
| 195 |
|
Ocular Motor Signs of Cerebellar Ataxia - Gaze-Evoked Nystagmus, Saccadic Pursuit, and VOR Supression | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 30-year-old woman with a several year long history of imbalance due to cerebellar ataxia of unclear etiology. Seen in this video are common ocular motor signs in patients with advanced cerebellar dysfunction inc... | Image/MovingImage |
| 196 |
 |
Oculogyric Crisis | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a patient with neuroleptic-induced oculogyric crisis. 𝗡𝗲𝘂𝗿𝗼-𝗼𝗽𝗵𝘁𝗵𝗮𝗹𝗺𝗼𝗹𝗼𝗴𝘆 𝗮𝗻𝗱 𝗡𝗲𝘂𝗿𝗼-𝗼𝘁𝗼𝗹𝗼𝗴𝘆 𝗧𝗲𝘅𝘁𝗯�... | Image/MovingImage |
| 197 |
 |
Oculopalatal Tremor and Internuclear Ophthalmoplegia Due to Hemorrhagic Pontine Cavernoma | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 60-year-old woman who experienced 2 episodes of vertigo, nausea and vomiting, which was felt to be related to recurrent hemorrhage of a pontine cavernoma that was adjacent to the fourth ventricle. The cavernoma ... | Image/MovingImage |
| 198 |
 |
Oculopalatal Tremor and One-and-a-Half Syndrome Due to Pontine Hemorrhage | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 65-year-old man who was put on a blood thinner, and shortly thereafter experienced a midline pontine hemorrhage, which was more dense on the left side. Immediately afterwards, right hemiparesis and hemi-anesthes... | Image/MovingImage |
| 199 |
 |
Oculopalatal Tremor with Prominent Nystagmus, Bilateral Horizontal Gaze Palsy, and Bilateral Facial Palsies | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 50-year-old woman who experienced the acute onset of right sixth and seventh nerve palsies and left hemiparesis. Two cavernomas within the right pons (one in the region of the facial colliculus) were demonstrat... | Image/MovingImage |
| 200 |
 |
Oculopalatal Tremor with Prominent Nystagmus, Bilateral Horizontal Gaze Palsy, and Bilateral Facial Palsies (Figure 1) | Figure 1, MRI T2 sequence demonstrating hyperintensities involving bilateral inferior olives of the medulla. This is a 50-year-old woman who experienced the acute onset of right sixth and seventh nerve palsies and left hemiparesis. Two cavernomas within the right pons (one in the region of the facia... | Image |