A collection of videos relating to the diagnosis and treatment of eye movement disorders. This collection includes many demonstrations of examination techniques.
Dan Gold, D.O., Associate Professor of Neurology, Ophthalmology, Neurosurgery, Otolaryngology - Head & Neck Surgery, Emergency Medicine, and Medicine, The Johns Hopkins School of Medicine.
A collection of videos relating to the diagnosis and treatment of eye movement disorders.
NOVEL: https://novel.utah.edu/
TO
Filters: Collection: "ehsl_novel_gold"
1 - 25 of 24
| Title | Description | Type | ||
|---|---|---|---|---|
| 1 |
 |
Enhanced Ptosis in Myasthenia Gravis | This is a 20-yo-woman who presented with generalized weakness, ptosis and ophthalmoplegia. She had severe ptosis OU at baseline, but when one eyelid was manually elevated, there was marked enhanced ptosis of the opposite eyelid. This was in accordance with Hering's law of equal innervation of the le... | Image/MovingImage |
| 2 |
 |
Bilateral Pseudo-abducens Palsies Due to Midbrain Stroke | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a man who suffered right>left midbrain strokes due to endocarditis complaining of ptosis and inability to move his eyes as well as hallucinations (peduncular hallucinosis). There was a presumed nuclear 3rd nerve p... | Image/MovingImage |
| 3 |
 |
Neuro-Ophthalmic Features and Pseudo-MG Lid Signs in Miller Fisher Syndrome | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 51-year-old woman who presented with imbalance, acute onset dizziness and diplopia that developed over three days following two weeks of upper respiratory infection and bacterial conjunctivitis. When she was ini... | Image/MovingImage |
| 4 |
 |
Typical Lid Signs (Cogan's Lid Twitch, Lid Hopping, Enhanced Ptosis) in Myasthenia Gravis | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 60-yo-woman with MG who displays typical eyelid signs including Cogan's lid twitch, lid hopping (appreciated during horizontal smooth pursuit in this patient), and enhanced ptosis in accordance with Hering's law... | Image/MovingImage |
| 5 |
 |
Miller Fisher Syndrome - Ophthalmoplegia, Ptosis and Ataxia | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a young man who presented with ptosis, difficulty moving the eyes and gait imbalance several weeks after a GI illness. Miller Fisher syndrome was diagnosed, IVIG therapy was initiated, and anti-Gq1b antibodies cam... | Image/MovingImage |
| 6 |
 |
Horner's Syndrome with Anhidrosis | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a patient with the onset of ptosis OD years prior, with clear evidence of a Horner's syndrome. Imaging of the oculosympathetic tract was unrevealing. The patient also mentioned that with exercise, the left side of... | Image/MovingImage |
| 7 |
 |
Neuro-Ophthalmic Features and Pseudo-MG Lid Signs in Miller Fisher Syndrome (Figure 1) | This is a 51-year-old woman who presented with imbalance, acute onset dizziness and diplopia that developed over three days following two weeks of upper respiratory infection and bacterial conjunctivitis. When she was initially seen as an outpatient, nystagmus was noted to the right and left, and a ... | Image |
| 8 |
 |
Test Your Knowledge - The Acute Vestibular Syndrome and Ptosis | What is the most likely localization in this patient presenting with vertical diplopia and acute onset prolonged vertigo? A. Right medial longitudinal fasciculus (MLF) B. Left medial longitudinal fasciculus C. Right medulla D. Left medulla E. Left midbrain A. Incorrect. A right MLF lesion (stroke, M... | Image/MovingImage |
| 9 |
 |
Apraclonidine Testing in Horner's syndrome | This patient experienced relatively abrupt ptosis and was seen and diagnosed with a Horner's syndrome within a few days of the onset. There were no other exam findings and history did not offer clues as to the etiology. Neuroimaging of the oculosympathetic tract was unrevealing. Apraclonidine testin... | Image/MovingImage |
| 10 |
 |
Bilateral INOs and Partial 3rd Nerve Palsies | This is a 45-year-old man with progressive ptosis and ophthalmoparesis. 10 years prior to presentation, he experienced diplopia and had a hyperintense lesion involving the medial longitudinal fasciculus (MLF) per report. Over time, he developed bilateral adduction paresis, ptosis and upgaze paresis ... | Image/MovingImage |
| 11 |
 |
The Acute Vestibular Syndrome with Dysarthria, Dysphagia, Dysphonia, Hemi-ataxia, and Saccadic Dysmetria Due to the Lateral Medullary (Wallenberg) Syndrome | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 50-year-old woman with the acute onset of vertigo, dysarthria, dysphagia and dysphonia/hoarseness (nucleus ambiguus), ptosis and imbalance. Her examination localized to a left lateral medullary (Wallenberg) synd... | Image/MovingImage |
| 12 |
 |
Chronic Progressive External Ophthalmoplegia (CPEO) and Cerebellar Signs | This is a 60-yo-woman who initially presented with imbalance and ophthalmoparesis. Initially, there was mild horizontal gaze limitation with mild gaze-evoked nystagmus and slow saccades, and over the years, gait ataxia and dysarthria (mainly a scanning quality to her speech) developed, and her ophth... | Image/MovingImage |
| 13 |
 |
Central 4th Nerve Palsy with Contralateral Horner's Syndrome | This is a 60-yo-woman who presented with a complaint of diplopia. Examination demonstrated a left hypertropia that worsened in right and down gaze as well as in left head tilt, and a left 4th nerve palsy was diagnosed. There was also evidence of a mild motility deficit in down/medial gaze OS, consis... | Image/MovingImage |
| 14 |
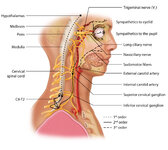 |
Figure 1: Oculosympathetic Pathway for Pupillary Dilation | The oculosympathetic tract is an uncrossed pathway that begins in the hypothalamus, with fibers descending in the brainstem (1st order, commonly affected in a lateral medullary syndrome), synapsing in the lower cervical/upper thoracic spinal cord (interomediolateral cell columns of C8-T2, also refer... | Image |
| 15 |
 |
Measuring Divergence Amplitude | Divergence insufficiency should be suspected in patients with binocular horizontal diplopia at distance (but not near) who lack abduction deficits. There should be an esodeviation greater at distance, and in older patients with levator dehiscence (or previous ptosis surgery) and prominent superior s... | Image/MovingImage |
| 16 |
 |
Light Near Dissociation in a Tonic Pupil | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 65-year-old woman who noticed difficulty reading and heightened sensitivity to lights OS for the last 6 months. On examination, there was mydriasis OS of about 6 mm (3 mm OD). The left (mydriatic) pupil constric... | Image/MovingImage |
| 17 |
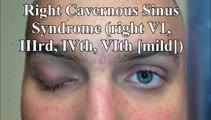 |
Cavernous Sinus Mass Causing Right 3rd and 4th Nerve Palsies | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: 25-yo-man who complained of diplopia and was initially found to have right 4th and 6th nerve palsies in the setting of a right cavernous sinus mass (subsequently diagnosed as Ewing's sarcoma). When seen in follow-up (this... | Image/MovingImage |
| 18 |
 |
Central (Nuclear) 3rd Nerve Palsies | Shown here are two patients with left sided midbrain pathology (hemorrhage and ischemia) which caused damage to the 3rd nucleus. Both of the patients have ipsilateral mydriasis, adduction, supra- and infraduction paresis. Ipsilateral>contralateral ptosis is also present, and localizes to the central... | Image/MovingImage |
| 19 |
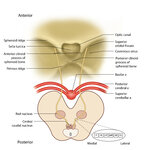 |
Figure 64: The Course of the 3rd (III) Nerve | The 3rd nucleus lies at the ventral border of the periaqueductal gray matter, at the level of the superior colliculus. In between the two nuclei is the midline central caudal nucleus (CCN), which innervates bilateral levator palpebrae muscles (explaining how a unilateral nuclear 3rd can cause bilate... | Image |
| 20 |
 |
Brainstem Ocular Motor Machinery | Seen here is a sagittal view of the brainstem. The medulla has a significant role in gaze-holding, and the nucleus prepositus hypoglossi (NPH, along with the medial vestibular nucleus ) is the horizontal neural integrator. The abducens (6th) nucleus is located in the dorsal pons, and sends off the 6... | Image/MovingImage |
| 21 |
 |
Vertical Gaze Palsy and Saccadic Intrusions Due to Anti-Ri from Head and Neck Carcinoma | A 55-yo- woman was admitted for imbalance and double vision. Three weeks prior to presentation she first noticed swelling on the right side of her face and neck. CT of the head and neck showed right-sided cervical adenopathy and enlarged left retropharyngeal node. Ultrasound- guided biopsy of the n... | Image/MovingImage |
| 22 |
 |
HINTS 'Plus' Patterns in the Acute Vestibular Syndrome Based on Location | HINTS ‘Plus' patterns in the acute vestibular syndrome based on location | Text |
| 23 |
|
Test Your Knowledge - Parinaud's Syndrome in Neurosarcoidosis | Watch the first segment of the video up to "Stop! What would you expect with vertical gaze?" and select the best response below. The patient also has mild right-beating nystagmus which can be ignored for the purposes of this question. A. The patient has pupillary findings consistent with bilateral 3... | Image/MovingImage |
| 24 |
|
Test Your Knowledge - Bilateral 4th Nerve Palsies | Watch the video until instructed to stop. Which of the following features is likely to be present given her exam findings? A. Gaze-evoked nystagmus and impaired smooth pursuit B. History of traumatic brain injury C. History of blepharoplasty or brow lift surgery and prominence of superior sulcus on ... | Image/MovingImage |
1 - 25 of 24