A collection of videos relating to the diagnosis and treatment of eye movement disorders. This collection includes many demonstrations of examination techniques.
Dan Gold, D.O., Associate Professor of Neurology, Ophthalmology, Neurosurgery, Otolaryngology - Head & Neck Surgery, Emergency Medicine, and Medicine, The Johns Hopkins School of Medicine.
A collection of videos relating to the diagnosis and treatment of eye movement disorders.
NOVEL: https://novel.utah.edu/
TO
| Title | Description | Type | ||
|---|---|---|---|---|
| 101 |
 |
Examples of Patients with Saccadic Intrusions (Square Wave Jerks) | Seen here are patients with saccadic intrusions that do have an intersaccadic interval. Square wave jerks are commonly seen in degenerative conditions, mainly involving the posterior fossa (e.g., cerebellar degeneration) and basal ganglia (e.g., progressive supranuclear palsy). | Image/MovingImage |
| 102 |
 |
Expanded Nystagmus & Saccadic Intrusions/Oscillations Differential | Expanded nystagmus & saccadic intrusions/ oscillations differential | Text |
| 103 |
 |
Eye Closure and Oculopalatal Tremor | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This patient suffered a traumatic brain injury with brainstem injury resulting in damage to Mollaret's triangle and palatal tremor. Inferior olivary hypertrophy was noted on her MRI, although no vertical and/or torsional ... | Image/MovingImage |
| 104 |
 |
Eye Handbook App for OKN | Optokinetic nystagmus (OKN): one way this can be examined virtually is using a smartphone application (e.g. Eye Handbook © app used in this video) or optokinetic tape/flag/drum held in front of the examiner's camera. The optokinetic stimulus should occupy the full screen of the patient's device (ea... | Image/MovingImage |
| 105 |
 |
Eyelid Anatomy | Seen here are the major muscles of eyelid opening and closure. The levator palpebrae, which is innervated by the oculomotor nerve, inserts on the tarsus via the levator aponeurosis and directly on the skin of the upper eyelid. The superior tarsal muscle (also known as Muller's muscle, which is inner... | Image |
| 106 |
 |
Eyelid Nystagmus | Lid nystagmus is a rhythmic eyelid movement commonly seen as an epiphenomenon of vertical nystagmus (typically upbeating, as in this case) due to a shared central pathway controlling elevation of the lid and supraduction. There can be isolated lid nystagmus if there is accompanying impairment of su... | Image/MovingImage |
| 107 |
 |
Figure 17: Bony Structures Relevant to the Orbit | The frontal, sphenoid, maxillary, ethmoid, and lacrimal bones make up the orbit. Structures passing through the optic canal include the optic nerve, oculosympathetic tract and ophthalmic artery. Structures passing through the superior orbital fissure include the superior ophthalmic vein, cranial ner... | Image |
| 108 |
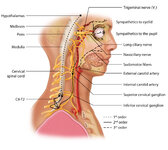 |
Figure 1: Oculosympathetic Pathway for Pupillary Dilation | The oculosympathetic tract is an uncrossed pathway that begins in the hypothalamus, with fibers descending in the brainstem (1st order, commonly affected in a lateral medullary syndrome), synapsing in the lower cervical/upper thoracic spinal cord (interomediolateral cell columns of C8-T2, also refer... | Image |
| 109 |
 |
Figure 24: Typical Visual Field Defects Associated with Discrete Lesions Along the Visual Pathways | Specific monocular or binocular visual field defects can be highly localizing when the neuroanatomy of the visual pathways is understood. The temporal visual field corresponds to the nasal retina, while the nasal visual field corresponds to the temporal retina. 1) Left optic nerve lesion - while an ... | Image |
| 110 |
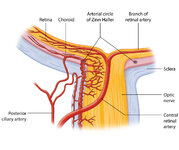 |
Figure 27: Vascular Supply of the Optic Nerve Head, Choroid and Retina | The ophthalmic artery is a branch of the internal carotid artery, which in turn, supplies the posterior ciliary (to choroid and outer retina) and central retinal (to inner retina) arteries. The central retinal artery (CRA) enters the optic nerve about 1 cm posterior to the globe, and an embolus may ... | Image |
| 111 |
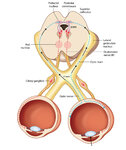 |
Figure 2: Parasympathetic Pathway for Pupillary Constriction | A bright light is shone in one eye, light enters the pupil and hyperpolarizes retinal photoreceptors which activates retinal ganglion cells. These signals propagate along the optic nerves, chiasm, optic tracts, and fibers responsible for the light reflex then synapse in the dorsal midbrain (prior to... | Image |
| 112 |
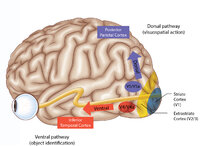 |
Figure 43: How the Brain Makes Sense of What It Sees - The Dorsal and Ventral Visual Pathways, and a 3 Tiered Approach to Vision | 1) Ventral ("what") stream - this begins with the ‘P' retinal ganglion cells à parvocellular layers of the lateral geniculate nucleus (LGN, 3-6) à V1/striate cortex (in blue) à V4/V4a (fusiform and lingual gyri) à occipitotemporal regions. 2) Dorsal ("where") stream - this begins with the ‘M... | Image |
| 113 |
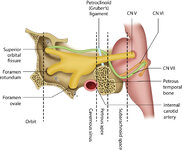 |
Figure 46: The Course of the 6th (VI) Nerve | The sixth nucleus is located dorsally, adjacent to the 4th ventricle, in the lower pons. The genu of the facial (7th) nerve wraps around the 6th nucleus, creating the facial colliculus, which bulges into the 4th ventricle. After the 6th nerve leaves the pons, it follows a vertical course along the c... | Image |
| 114 |
 |
Figure 50: Anatomy and Physiology of the Saccadic Pathways | When a saccade is desired (or reflexively triggered), signals project from the saccade-related cortical eye fields to the superior colliculus, which serves to integrate and relay commands to the saccade generating brainstem circuitry. The inferior cerebellar peduncle (ICP) carries climbing fibers to... | Image |
| 115 |
 |
Figure 51: Lateral Medullary Lesion Causing Saccadic Dysmetria | A lesion of the left lateral medulla and inferior cerebellar peduncle (ICP) will cause decreased climbing fiber inhibition of the left dorsal vermis causing simple-spike (inhibitory) discharge of Purkinje cells to increase. Increased Purkinje cell firing leads to increased inhibition of the ipsilate... | Image |
| 116 |
 |
Figure 53: Vascular Distribution and Anatomy Relevant to the Lateral Medullary (Wallenberg) Syndrome | This axial section of the medulla highlights those structures that, when damaged, are responsible for the vestibular and ocular motor features of the Wallenberg syndrome. The nucleus prepositus hypoglossi (NPH) and medial vestibular nucleus (MVN) complex is important for horizontal gaze-holding (neu... | Image |
| 117 |
 |
Figure 61: Vascular Distribution and Anatomy (Including 6th, 7th, 8th Nerves, MLF) of the Pons | In this axial section of the pons, the proximity of the 7th (VII) and 8th (VIII) fascicles can be appreciated, and a lateral inferior pontine syndrome (anterior inferior cerebellar artery, AICA territory), which could involve both of these fascicles, could cause acute prolonged vertigo accompanied b... | Image |
| 118 |
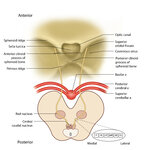 |
Figure 64: The Course of the 3rd (III) Nerve | The 3rd nucleus lies at the ventral border of the periaqueductal gray matter, at the level of the superior colliculus. In between the two nuclei is the midline central caudal nucleus (CCN), which innervates bilateral levator palpebrae muscles (explaining how a unilateral nuclear 3rd can cause bilate... | Image |
| 119 |
 |
Figure 65: Vascular Distribution and Anatomy (Including 3rd Nerve) of the Rostral Midbrain | In this axial section of the midbrain at the level of the superior colliculus, the paired 3rd nuclei are located ventral to the periaqueductal grey, and the midline central caudal nucleus (CCN) is located in between. The fascicles that exit the IIIrd nuclei carry the fibers destined to innervate the... | Image |
| 120 |
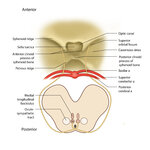 |
Figure 68: The Course of the 4th (IV) Nerve | The 4th nucleus lies at the ventral border of the periaqueductal gray matter, at the level of the inferior colliculus. The fascicles exit the nucleus dorsally and decussate at the anterior medullary velum (anterior floor of the fourth ventricle), and then exit the brainstem dorsally. The peripheral ... | Image |
| 121 |
 |
Figure 69: Vascular Distribution and Anatomy (Including 4th Nerve) of the Caudal Midbrain | In this axial section of the midbrain at the level of the inferior colliculus, the 4th nuclei are located ventral to the periaqueductal grey, dorsal to the medial longitudinal fasciculus (MLF) and medial to the oculosympathetic tract. Fascicles exit the nucleus dorsally and decussate at the anterior... | Image |
| 122 |
 |
Figure 80: Vascular Distribution and Anatomy Relevant to the Medial Medullary Syndrome | This axial section of the medulla highlights those structures that, when damaged, are often responsible for spontaneous upbeat nystagmus (UBN). The nucleus of Roller and nucleus intercalatus normally have an inhibitory influence over the cerebellar flocculus, and when there is a lesion of Roller/int... | Image |
| 123 |
 |
Five Common Ocular Motor Signs in Cerebellar Disorders - Saccadic Hypermetria, Saccadic Pursuit & VOR Suppression, Gaze-evoked & Rebound Nystagmus | (1) Saccadic hypermetria - an overshoot of the visual target (2) Saccadic smooth pursuit - due to impaired pursuit and low gain, saccades are needed to keep up with the visual target. This gives it a ‘choppy' appearance. (3) Saccadic vestibulo-ocular reflex (VOR) suppression - another... | Image/MovingImage |
| 124 |
 |
Fixation and Gaze Holding | Fixation and gaze-holding: assess for nystagmus or saccadic intrusions by observing the eyes in primary position. Then instruct the patient to look in each position of gaze, and to hold that position to assess for gaze-evoked nystagmus. In doing so, motility can also be evaluated with both eyes view... | Image/MovingImage |
| 125 |
 |
The Gans Maneuver for Right Posterior Canal Benign Paroxysmal Positional Vertigo | This maneuver is recommended for individuals with cervical restrictions or precautions, as the maneuver avoids cervical hyperextension and may reduce cervical pain associated with repositioning maneuvers. The Epley maneuver has higher subjective and objective success rates compared to the Gans maneu... | Text |