A collection of videos relating to the diagnosis and treatment of eye movement disorders. This collection includes many demonstrations of examination techniques.
Dan Gold, D.O., Associate Professor of Neurology, Ophthalmology, Neurosurgery, Otolaryngology - Head & Neck Surgery, Emergency Medicine, and Medicine, The Johns Hopkins School of Medicine.
A collection of videos relating to the diagnosis and treatment of eye movement disorders.
NOVEL: https://novel.utah.edu/
TO
Filters: Collection: "ehsl_novel_gold"
| Title | Description | Type | ||
|---|---|---|---|---|
| 51 |
 |
Demonstration of HINTS Examination in a Normal Subject | In the acute vestibular syndrome - consisting of acute prolonged vertigo, spontaneous nystagmus, imbalance, nausea/vomiting, head motion intolerance which is typically due to vestibular neuritis or posterior fossa stroke - a 3 step test of ocular motor and vestibular function known as HINTS, has hig... | Image/MovingImage |
| 52 |
 |
Dynamic Visual Acuity | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: After assessing static binocular visual acuity, dynamic visual acuity (DVA) is determined by repeating the test during horizontal and vertical head shaking at 2-3 Hz. Dynamic visual acuity is most important to test when ... | Image/MovingImage |
| 53 |
 |
How to Measure Ocular Alignment Virtually | Ocular alignment: the alternate cover test can be performed by instructing the patient to hold their head steady, fix their eyes on the camera (or a more distant target - the closer the fixation target, the more of an exodeviation the examiner will see), and use their cell phone (or a spoon) to occl... | Image/MovingImage |
| 54 |
 |
Modified (Chair) Dix-Hallpike | The safety of the patient should be prioritized when completing this test virtually, and the examiner should avoid putting the patient in a position where a fall may occur. Modified (chair) Dix-Hallpike:(1) this test can be used for patients who may not be able to safely undertake the traditional Di... | Image/MovingImage |
| 55 |
 |
Pressure Testing for Superior Canal Dehiscence Syndrome | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: Superior semicircular canal dehiscence syndrome (SCDS) is caused by a third mobile window in the inner ear. This allows for transmission of sound or pressure to the superior canal. Tragal compression and/or glottic and ... | Image/MovingImage |
| 56 |
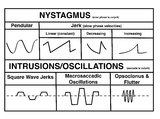 |
A Comparison of Nystagmus and Saccadic Intrusions/Oscillations | Nystagmus can be classified into pendular and jerk waveforms, where both are generated by a slow, pathologic phase. Corrective phase (the position reset mechanism) differs. In pendular nystagmus, the eyes move back and forth with about the same velocity and amplitude, similar to that of a pendulum... | Image |
| 57 |
 |
Active Head Impulse Test | Active head impulse test (HIT): instruct the patient to fix their eyes on the camera and turn their head 20o to the right/left, and then make a rapid movement toward the midline to align their head with the camera again, keeping their eyes fixed on the camera throughout. A simple instruction is to a... | Image/MovingImage |
| 58 |
 |
Dix-Hallpike | The safety of the patient should be prioritized when completing this test virtually, and the examiner should avoid putting the patient in a position where a fall may occur. Floor (or bed) Dix-Hallpike: this test can be used for patients who are fully mobile and able to get down to the floor and up a... | Image/MovingImage |
| 59 |
 |
Eye Handbook App for OKN | Optokinetic nystagmus (OKN): one way this can be examined virtually is using a smartphone application (e.g. Eye Handbook © app used in this video) or optokinetic tape/flag/drum held in front of the examiner's camera. The optokinetic stimulus should occupy the full screen of the patient's device (ea... | Image/MovingImage |
| 60 |
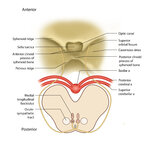 |
Figure 51: Lateral Medullary Lesion Causing Saccadic Dysmetria (Supplement) | Image | |
| 61 |
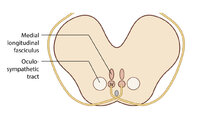 |
Figure 51: Lateral Medullary Lesion Causing Saccadic Dysmetria (Supplement) | Image | |
| 62 |
 |
Figure 64: The Course of the 3rd (III) Nerve (Supplement) | Image | |
| 63 |
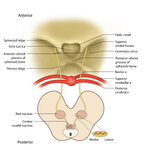 |
Figure 68: The Course of the 4th (IV) Nerve (Supplement) | Image | |
| 64 |
 |
Visual Sensitivity | Image/MovingImage | |
| 65 |
 |
Horizontal Canal - BPPV: Gufoni for Right Apogeotropic | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: To treat the right apogeotropic (beating towards the sky with right ear down and with left ear down - e.g., left beating nystagmus with right supine roll test or with right ear down; right beating nystagmus with left supi... | Image/MovingImage |
| 66 |
 |
Posterior Canal - BPPV: Epley and Semont Maneuvers | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: Epley/canalith repositioning maneuver (CRP) To treat right posterior canal (PC)-BPPV (each position maintained for at least 30 seconds or until nystagmus and/or vertigo cease): • First the patient is placed in the long-... | Image/MovingImage |
| 67 |
 |
Figure 53: Vascular Distribution and Anatomy Relevant to the Lateral Medullary (Wallenberg) Syndrome (Supplement) | Image | |
| 68 |
 |
Figure 53: Vascular Distribution and Anatomy Relevant to the Lateral Medullary (Wallenberg) Syndrome (Supplement) | Image | |
| 69 |
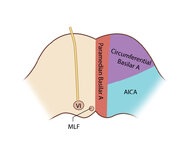 |
Figure 61: Vascular Distribution and Anatomy (Including 6th, 7th, 8th Nerves, MLF) of the Pons (Supplement) | Image | |
| 70 |
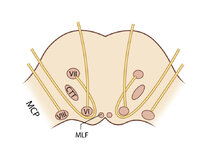 |
Figure 61: Vascular Distribution and Anatomy (Including 6th, 7th, 8th Nerves, MLF) of the Pons (Supplement) | Image | |
| 71 |
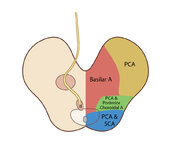 |
Figure 65: Vascular Distribution and Anatomy (Including 3rd Nerve) of the Rostral Midbrain (Supplement) | Image | |
| 72 |
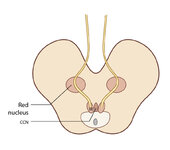 |
Figure 65: Vascular Distribution and Anatomy (Including 3rd Nerve) of the Rostral Midbrain (Supplement) | Image | |
| 73 |
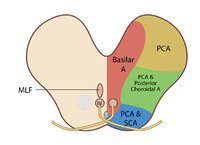 |
Figure 69: Vascular Distribution and Anatomy (Including 4th Nerve) of the Caudal Midbrain (Supplement) | Image | |
| 74 |
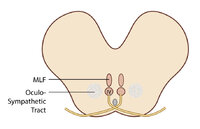 |
Figure 69: Vascular Distribution and Anatomy (Including 4th Nerve) of the Caudal Midbrain (Supplement) | Image | |
| 75 |
 |
Figure 80: Vascular Distribution and Anatomy Relevant to the Medial Medullary Syndrome (Supplement) | Image |