The Health Education Assets Library (HEAL) is a collection of over 22,000 freely available digital materials for health sciences education. The collection is now housed at the University of Utah J. Willard Marriott Digital Library.
TO
Filters: Collection: ehsl_heal
| Title | Description | Subject | Collection | ||
|---|---|---|---|---|---|
| 201 |
 |
RBBB: Precordial leads | RBBB: Precordial leads | Knowledge Weavers ECG | |
| 202 |
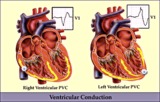 |
RV vs LV PVC's - marquette | RV vs LV PVC's - marquette | Knowledge Weavers ECG | |
| 203 |
 |
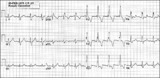
Rate-dependent LBBB | In this rhythm strip of sinus arrhythmia, the faster rates have a LBBB morphology. In some patients with a diseased left bundle branch, the onset of LBBB usually occurs initially as a rate-dependent block; i.e., the left bundle fails to conduct at the faster rate because of prolonged refractoriness... | Knowledge Weavers ECG | |
| 204 |
 |
Right Atrial Enlargement (RAE) & Right Ventricular Hypertrophy (RVH) | RAE is recognized by the tall (>2.5mm) P waves in leads II, III, aVF. RVH is likely because of right axis deviation (+100 degrees) and the Qr (or rSR') complexes in V1-2. | Knowledge Weavers ECG | |
| 205 |
 |
Right Axis Deviation & RAE (P pulmonale): Leads I, II, III | Right Axis Deviation & RAE (P pulmonale): Leads I, II, III | Knowledge Weavers ECG | |
| 206 |
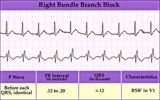 |
Right Bundle Branch Block | Right Bundle Branch Block | Knowledge Weavers ECG | |
| 207 |
 |
Right Ventricular Hypertrophy (RVH) & Right Atrial Enlargement (RAE) | In this case of severe pulmonary hypertension, RVH is recognized by the prominent anterior forces (tall R waves in V1-2), right axis deviation (+110 degrees), and P pulmonale (i.e., right atrial enlargement). RAE is best seen in the frontal plane leads; the P waves in lead II are >2.5mm in amplitud... | Knowledge Weavers ECG | |
| 208 |
 |
Right axis deviation: QRS axis = +130 degrees | Lead aVR is almost isoelectric; lead I is mostly negative, and lead III is very positive. The QRS axis, therefore, is +130 degrees. Note that the slightly more positive AVR moves the axis slightly beyond +120 degrees; i.e., closer to the + pole of the aVR lead. | Knowledge Weavers ECG | |
| 209 |
 |
Right bundle branch block (RBBB) | Right bundle branch block (RBBB) | Knowledge Weavers ECG | |
| 210 |
 |
SA exit block - marquette | SA exit block - marquette | Knowledge Weavers ECG | |
| 211 |
 |
ST segment depression | ST segment depression is a nonspecific abnormality that must be evaluated in the clinical context in which it occurs. In a patient with angina pectoris ST depression usually means subendocardial ischemia and, unlike ST elevation, is not localizing to a particular coronary artery lesion. | Knowledge Weavers ECG | |
| 212 |
 |
ST segment depression: precordial leads | ST segment depression: precordial leads | Knowledge Weavers ECG | |
| 213 |
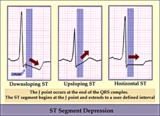 |
ST segment diagram - marquette | ST segment diagram - marquette | Knowledge Weavers ECG | |
| 214 |
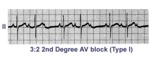 |
Second degree AV block, type I, with 3:2 conduction ratio | There are two types of 2nd degree AV Block. In this example of Type I or Wenckebach AV block there are 3 P waves for every 2 QRSs; the PR interval increases until a P wave fails to conduct. This is an example of group beating. | Knowledge Weavers ECG | |
| 215 |
 |
Second degree AV block, type I, with bradycardia-dependent RBBB | An interesting and unusual form of rate-dependent bundle branch block. Normal sinus rhythm at 85 bpm is present with a 3:2 and 2:1 2nd degree AV block. The progressive PR prolongation in the 3:2 block makes this a type-I or Wenckebach block.Long cycles end in RBBB; short cycles have normal QRS dur... | Knowledge Weavers ECG | |
| 216 |
 |
Sino-atrial exit block, type I or wenckebach | This example illustrates 2nd degree sino-atrial exit block. In type 1 S-A block the conduction time between sinus firing and atrial capture progressively prolong, but this cannot be seen on the ECG tracing; type I exit block is inferred if the P-P intervals gradually shorten before the pause and if... | Wenckebach AV Block; Ladder Diagram | Knowledge Weavers ECG |
| 217 |
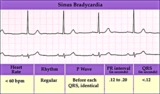 |
Sinus bradycardia | Sinus bradycardia | Knowledge Weavers ECG | |
| 218 |
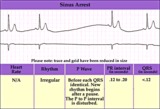 |
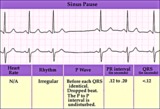
Sinus pause or arrest - marquette | Sinus pause or arrest - marquette | Knowledge Weavers ECG | |
| 219 |
 |
Sore thumbs | Two funny looking premature beats are seen in this rhythm strip. Beat A is preceded by a PAC which distorts the T wave, making this an aberrantly conducted PAC. Beat B is a PVC. The notch on the down slope of the QRS complex clearly identifies this as a PVC and not aberrancy. | Knowledge Weavers ECG | |
| 220 |
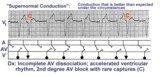 |
Supernormal conduction: 2nd degree AV block with rare captures; accelerated ventricular rhythm | This complicated rhythm strip illustrates 'supernormal' conduction... a situation where conduction is better than expected. The ladder diagram shows that the accelerated ventricular rhythm prevents most of the sinus impulses from reaching the ventricles. Only appropriately timed sinus impulses rea... | Knowledge Weavers ECG | |
| 221 |
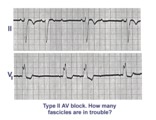 |
Trifascicular block: RBBB, LAFB, and mobitz II 2nd degree AV block | A nice example of trifascicular block: Lead V1 shows RBBB; Lead II is mostly negative with an rS morphology suggesting left anterior fascicular block. Since Mobitz II 2nd degree AV block is more often located in the bundle branch system, the only location left for this block is the left posterior ... | Knowledge Weavers ECG | |
| 222 |
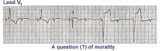 |
Two Wrongs Sometimes Make a Right | The question mark is over a normal looking QRS that occurs during 2:1 AV block with RBBB. Following this QRS a ventricular escape rhythm takes over. The normal looking beat is actually a fusion beat resulting from simultaneous activation of the ventricles; the sinus impulse enters the left ventric... | Knowledge Weavers ECG | |
| 223 |
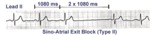 |
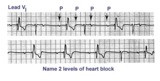
Type II, 2nd degree sino-atrial block | Two types of 2nd degree SA block have been described. In type-I, or SA Wenckebach, the P-P interval of the pause is less than 2x the preceding P-P intervals. In type-II SA block the P-P interval of the pause is approximately 2x the normal P-P interval. The distinction between types I and II is no... | Knowledge Weavers ECG | |
| 224 |
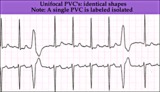 |
Unifocal PVCs - marquette | Unifocal PVCs - marquette | Knowledge Weavers ECG | |
| 225 |
 |
Ventricular Pacemaker Rhythm: V1-3 | Note the small pacemaker spikes before the QRS complexes. In addition, the QRS complex in V1-3 exhibits ventricular ectopic morphology; i.e., there is a slur or notch at the beginning of the S wave, and >60ms delay from onset to QRS to nadir of S wave. This rules against a supraventricular rhythm wi... | Knowledge Weavers ECG |