The Health Education Assets Library (HEAL) is a collection of over 22,000 freely available digital materials for health sciences education. The collection is now housed at the University of Utah J. Willard Marriott Digital Library.
TO
| Title | Description | Subject | Collection | ||
|---|---|---|---|---|---|
| 201 |
 |
Ventricular tachycardia with retrograde wenckebach | Approximately 50 percent of ventricular tachycardias are associated with AV dissociation. The other 50 percent have retrograde atrial capture. This example shows ventricular tachycardia with retrograde Wenckebach. The retrograde P waves are hard to find, but the arrows are of some help. | Wenckebach AV Block | Knowledge Weavers ECG |
| 202 |
 |
Nonconducted and aberrantly conducted PAC's | In A the slow sinus rhythm is actually caused by nonconducted PACs hidden in the ST segment. This is confirmed in B where some of the PACs are aberrantly conducted with LBBB, and some PACs are nonconducted. | Knowledge Weavers ECG | |
| 203 |
 |
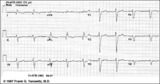
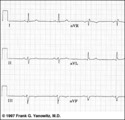
Left anterior fasicular block: frontal plane leads | Left anterior fascicular block, LAFB, is recognized by left axis deviation of -45 degrees or greater; rS complexes in II, III, aVF; and a small Q wave in I and/or aVL. | Knowledge Weavers ECG | |
| 204 |
 |
Right bundle branch block (RBBB) | Right bundle branch block (RBBB) | Knowledge Weavers ECG | |
| 205 |
 |
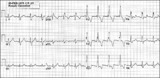
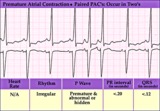
All about premature beats | All about premature beats | Knowledge Weavers ECG | |
| 206 |
 |
Inferoposterior MI | Inferoposterior MI | Knowledge Weavers ECG | |
| 207 |
 |
Neural Network Controlling Wakefulness (Labeled) | Brainstem reticular activating system. | Royal College of Surgeons in Ireland Illustrations | |
| 208 |
 |
Sino-atrial exit block, type I or wenckebach | This example illustrates 2nd degree sino-atrial exit block. In type 1 S-A block the conduction time between sinus firing and atrial capture progressively prolong, but this cannot be seen on the ECG tracing; type I exit block is inferred if the P-P intervals gradually shorten before the pause and if... | Wenckebach AV Block; Ladder Diagram | Knowledge Weavers ECG |
| 209 |
 |
Inferior & Anteroseptal MI + RBBB | Pathologic Q waves are seen in leads II, III, aVF (inferior MI) and in leads V1-3 (anteroseptal MI). RBBB is recognized by the wide QRS (>0.12s) and the anterior/rightwards orientation of terminal QRS forces. When an anteroseptal MI complicates RBBB (or visa versa) the rSR' complex in V1 (typical ... | Knowledge Weavers ECG | |
| 210 |
 |
Atrial flutter with 3:2 conduction ratio: frontal plane leads | Note the subtle bigeminy in the RR intervals. The best way to identify the flutter waves in this example is to imagine what lead III would look like if the QRS complexs disappeared; what remains is a reasonable saw-tooth pattern characteristic of atrial flutter with a flutter rate of about 300 bpm... | Knowledge Weavers ECG | |
| 211 |
 |
Accelerated ventricular rhythm with retrograde atrial capture and echo beats | Retrograde atrial captures from an accelerated ventricular focus are occurring with increasing R-P intervals, When the longer R-P occurs, the impulse traversing the AV junction finds a route back to the ventricles, and the result is a ventricular echo. | Knowledge Weavers ECG | |
| 212 |
 |
Folate Pool - The Role of B Vitamins in One-Carbon Metabolism | This figure depicts the pathway for folate utilization and the role of vitamins B6 and B12 in the metabolism of methyl-tetrahydrofolate and homocysteine. | Folate; Folicin | HEAL Open Review Collection |
| 213 |
 |
ECG components diagram - marquette | ECG components diagram - marquette | Knowledge Weavers ECG | |
| 214 |
 |
Postero-lateral MI: Precordial Leads | Postero-lateral MI: Precordial Leads | Knowledge Weavers ECG | |
| 215 |
 |
Indeterminate frontal plane QRS axis | Indeterminate frontal plane QRS axis | Knowledge Weavers ECG | |
| 216 |
 |
PAC couplet - marquette | PAC couplet - marquette | Knowledge Weavers ECG | |
| 217 |
 |
Normal variant: Early repolarization | Early repolarization, a misnomer, describes a pattern of localized or diffuse ST segment elevation. This is especially seen in leads with prominent R waves. In this example leads I, II, V5 and V6 illustrate the early repolarization pattern. ST segments usually have a concave upwards pattern and ta... | Knowledge Weavers ECG | |
| 218 |
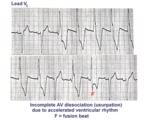 |
AV dissociation by usurpation | Normal sinus rhythm is interrupted by an accelerated ventricular rhythm whose rate is slightly faster than the sinus rhythm. Fusion QRS complexes occur whenever the sinus impulse enters the ventricles at the same time the ectopic ventricular focus initiates its depolarization. | Knowledge Weavers ECG | |
| 219 |
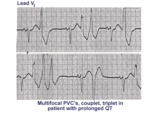 |
Long QT mischief | The long QT ECG has many causes: electrolyte abnormalities including hypo-K, hypo-Mg, and hypo-Ca; drugs including type I antiarrhythmics; CNS injury; and hereditary syndromes. Ventricular arrhythmias are thought to be caused by afterdepolarizations or triggered automaticity. | Knowledge Weavers ECG | |
| 220 |
 |
Nonconducted and conducted PAC's | The pause in this example is the result of a nonconducted PAC, as indicated by the first arrow. The second arrow points to a conducted PAC. The most common cause of an unexpected pause in rhythm is a nonconducted PAC. | Knowledge Weavers ECG | |
| 221 |
 |
Atypical LBBB with Q waves in leads I and aVL | In typical LBBB, there are no initial Q waves in leads I, aVL, and V6. If Q waves are present in 2 or more of these leads, myocardial infarction is present. | Knowledge Weavers ECG | |
| 222 |
 |
Old inferior MI, PVCs, and atrial fibrillation | Old inferior MI, PVCs, and atrial fibrillation | Knowledge Weavers ECG | |
| 223 |
 |
Frontal plane QRS axis = -45 degrees | Frontal plane QRS axis = -45 degrees | Knowledge Weavers ECG | |
| 224 |
 |
Fatty acyl CoA elongation in the endoplasmic reticulum | This shows the overall process of fatty acyl elongation in the endoplasmic reticulum. The process resembles that catalyzed by fatty acyl synthase, but the individual activities appear to be on separate enzymes. | Knowledge Weavers Fatty Acids | |
| 225 |
 |
LVH & PVCs: Precordial Leads | LVH & PVCs: Precordial Leads | Knowledge Weavers ECG |