The Health Education Assets Library (HEAL) is a collection of over 22,000 freely available digital materials for health sciences education. The collection is now housed at the University of Utah J. Willard Marriott Digital Library.
TO
Filters: Collection: "ehsl_heal"
| Title | Description | Subject | Collection | ||
|---|---|---|---|---|---|
| 801 |
 |
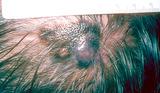
Rosacea | The typical appearance of a patient with rosacea. The patient usually has underlying erythema on the nose and cheeks, and generally has superimposed red papules and pustules on these areas. The first stage of rosacea consists of only erythema, and the second stage consists of the superimposed red pa... | Knowledge Weavers Dermatology | |
| 802 |
 |
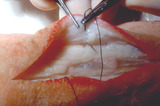
Excision: suturing | A single loop is thrown around the needle holder. The short arm of the suture is then grasped. | Knowledge Weavers Dermatology | |
| 803 |
 |
Suturing | This demonstrates a single loop of suture thrown around the needle holder. | Knowledge Weavers Dermatology | |
| 804 |
 |
Epinephrine | If a patient is on beta-blockers and experiences severe urticaria or anaphylaxis, often epinephrine does not work. Glucagon can be used in lieu of epinephrine, and generally 1 mg (regardless of body size) is given in the subcutaneous fat | Knowledge Weavers Dermatology | |
| 805 |
 |
Punch biopsy | I gently lift the punch without pinching it and thereby creating damage to the specimen, and then snip the fatty strand that connects the skin to the underlying fat and muscle. | Knowledge Weavers Dermatology | |
| 806 |
 |
Suturing | With the needle holders placed inside the long arm (needle bearing end) of V, and | Knowledge Weavers Dermatology | |
| 807 |
 |
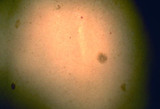
Pubic lice | Pubic lice. They are 1-2 mm diameter and are visible with the naked eye. | Knowledge Weavers Dermatology | |
| 808 |
 |
Head lice | On close inspection one could often see the adult lice as shown here. | Knowledge Weavers Dermatology | |
| 809 |
 |
Excision procedure | This demonstrates the 45 degree angle in cross-section. | Knowledge Weavers Dermatology | |
| 810 |
 |
Pemphigus | This patient has pemphigus. In this disease, there are antibodies produced against components of the materials that hold the epidermal cells together, and the epidermis breaks apart within the mid-epidermal level. | Knowledge Weavers Dermatology | |
| 811 |
 |
Seborrheic keratoses | One month after freezing seborrheic keratoses showing slight residual inflammation and postinflammatory hyperpigmentation. This generally resolves within several months after the procedure. | Knowledge Weavers Dermatology | |
| 812 |
 |
Micrograph of the base of hair follicle | An electron micrograph of the base of hair follicle. The epidermal papilla, shown at the bottom center, controls the growth rate of the hair follicle. | Knowledge Weavers Dermatology | |
| 813 |
 |
Melanoma | Melanoma in the scalp of a patient approximately 65-years-old. | Knowledge Weavers Dermatology | |
| 814 |
 |
Ingrown nail | This demonstrates local infiltration of the skin around the nail. It is crucial to inject slowly and to advance the needle slowly. I found local infiltration to be superior to a digital block. | Knowledge Weavers Dermatology | |
| 815 |
 |
Capillary hemangiomas | The red papules are benign vascular growths called capillary hemangiomas. | Knowledge Weavers Dermatology | |
| 816 |
 |
Spider telangiectasia | The red lesion on the nose is a spider telangiectasia. | Knowledge Weavers Dermatology | |
| 817 |
 |
Fleas | The flea. These have been shown to live up to 40 days without a blood meal. The major disease we see in the Intermountain West that is carried by fleas is plague, and this is actually seen very rarely. | Knowledge Weavers Dermatology | |
| 818 |
 |
Scalpel | This shows the scalpel, handle and blade. Note that the angle at the base of the blade, as well as the ankle at the attachment base of the scalpel handle should be the same. | Knowledge Weavers Dermatology | |
| 819 |
 |
Suturing | The short and (non-needle bearing end) of the suture is then grasped with the needle holder, and the suture is pulled taut forming a double loop as shown here in cross-section. One cannot tighten the suture by pulling across the wound, and | Knowledge Weavers Dermatology | |
| 820 |
 |
Wound culturing | If the tissue around the wound is red and tender suggesting infection, then the wound should be cultured. The best mode of culture of a long-standing wound is to actually biopsy tissue at the base of the wound and culture that tissue. | Knowledge Weavers Dermatology | |
| 821 |
 |
Body louse | Body louse. They are several mm long and therefore visible with the naked eye. | Knowledge Weavers Dermatology | |
| 822 |
 |
Cotton gauze | The topical antibiotic and non-adherent dressing are secured in place with tape or a cotton gauze wrap. The third principle of wound care is to ensure good nutrition, and the most important element of that would be to keep pressure off the wound, particularly if the patient is immobilized and can't ... | Knowledge Weavers Dermatology | |
| 823 |
 |
Suturing | This demonstrates in cross-sectional view the placement of the deep dermal suture. | Knowledge Weavers Dermatology | |
| 824 |
 |
Suturing | The needle holder is placed on the inside of the long arm (needle bearing end) of the V, and the suture is wrapped twice around the needle holder. | Knowledge Weavers Dermatology | |
| 825 |
 |
Suturing | This demonstrates cutting the deep dermal suture just above the knot. | Knowledge Weavers Dermatology | |
| 826 |
 |
Electrocautery | This shows the biopsy site after light electrocautery. | Knowledge Weavers Dermatology | |
| 827 |
 |
Seborrheic dermatitis | Seborrheic dermatitis involving the beard. | Knowledge Weavers Dermatology | |
| 828 |
 |
Electrocautery | Very light electrocautery can be used to smooth any uneven edges. If using the hyfrecator model, it should be plugged into low and a setting of 30 on the older machines, or setting of 3 watts on the newer machines should be used, and a very light brush kind of stroke should be used to smooth out the... | Knowledge Weavers Dermatology | |
| 829 |
 |
Suturing | The other side of the wound is then rolled open to expose the underlying dermis, and I placed the suture in the under-portion of the dermis as far away from the wound edge as possible. I enter from the side where the wound center, and then exit away from the wound center. | Knowledge Weavers Dermatology | |
| 830 |
 |
Excision: suturing | Two loops are placed around the needle holder to initiate the first throw. The short end of the suture is then grasped, and the hand holding the long(needle bearing) end of the suture crosses over the hand with the needle holder. | Knowledge Weavers Dermatology | |
| 831 |
 |
Excision procedure | Deep dermal suture is placed as far away from the wound edge as possible. It's initiated on the non-dominant (left) side, and final exit is on the dominant (right) side as shown here. | Knowledge Weavers Dermatology | |
| 832 |
 |
Lamellar ichthyosis | Lamellar ichthyosis. The abnormal stratum corneum has produced what appears as very thick scale on the skin, and with an abnormal barrier layer these patients commonly get secondary staphylococcal and yeast infections. Note that there are other associated ectodermal problems such as the teeth, hair,... | Knowledge Weavers Dermatology | |
| 833 |
 |
Scabies | A nursing home patient who was infested with scabies. Shows the typical pruritic red papules in the axilla. | Knowledge Weavers Dermatology | |
| 834 |
 |
Ingrown nail | This shows the nail plate and part of the attached matrix having been removed. | Knowledge Weavers Dermatology | |
| 835 |
 |
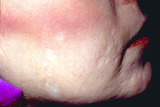
Atopic dermatitis | Atopic dermatitis (eczema) involving the cheeks of a child. | Knowledge Weavers Dermatology | |
| 836 |
 |
Suturing | As the suture exits from the wound, the ends of the suture can be lifted to form aV. The long arm of the V is formed by the needle bearing end of the suture. | Knowledge Weavers Dermatology | |
| 837 |
 |
Epinephrine | Epinephrine also comes in a crystalline form, and the brand name is Sus-Phrine. This is a Depo form of epinephrine. | Knowledge Weavers Dermatology | |
| 838 |
 |
mosquito | Mosquitos are not known to be vectors for significant diseases in Utah. | Knowledge Weavers Dermatology | |
| 839 |
 |
Spider telangiectasia | A spider telangiectasia is compressible and blanchable with adequate pressure. Generally, as the pressure is released the central feeding vessel can be seen and often pulsates. | Knowledge Weavers Dermatology | |
| 840 |
 |
Hair regrowth | Rogaine helps to restore hair regrowth of some degree in about a third of men. | Dermatology; Hair | Knowledge Weavers Dermatology |
| 841 |
 |
Suturing | The needle is then reversed on the needle holder, and I then enter the wound edge as closely and superficially as possible, and | Knowledge Weavers Dermatology | |
| 842 |
 |
Androgenetic alopecia | Androgenetic alopecia often induces fine curly hair along the lateral margins of the scalp. | Knowledge Weavers Dermatology | |
| 843 |
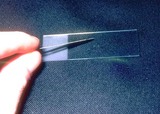 |
Scale and mineral oil are applied to a slide | The scale and mineral oil are applied to a slide. | Knowledge Weavers Dermatology | |
| 844 |
 |
Eversion of a wound | This shows eversion of the wound on the face of a young man. Most of the eversion is created by the deep dermal suture, and not by the superficial sutures shown here. The upper epidermis and dermis were closed here using 4-0 Prolene. It simply provides some stability to the edges of the wound so tha... | Knowledge Weavers Dermatology | |
| 845 |
 |
Atopic dermatitis in children | Atopic dermatitis often involves the hand and/or feet. | Knowledge Weavers Dermatology | |
| 846 |
 |
Insect bite reaction | This represents an exaggerated insect bite reaction with her other striking erythema surrounding the papules. | Knowledge Weavers Dermatology | |
| 847 |
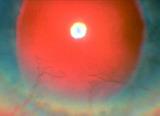 |
Neovascularization of the cornea secondary to rosacea | Neovascularization of the cornea secondary to rosacea. | Knowledge Weavers Dermatology | |
| 848 |
 |
Deep dermal suture | This demonstrates the placement of the deep dermal suture. Note that the deep dermal suture is placed as far away from the wound edge as possible to avoid compromise of blood flow to the wound. This demonstrates the exit of the deep dermal suture ends from the wound. Note that the order is loop, the... | Knowledge Weavers Dermatology | |
| 849 |
 |
Dr. Maxwell M. Wintrobe | Dr. Maxwell M. Wintrobe told us as medical students to put ourselves in the position of the patient and try to imagine what it would be like to be the recipient of some of the procedures that we do to them. He was a great advocate of empathy. | Knowledge Weavers Dermatology | |
| 850 |
 |
Pitted scarring secondary to small inflammatory acne lesions | Pitted scarring secondary to small inflammatory acne lesions. | Knowledge Weavers Dermatology | |
| 851 |
 |
Basal cell carcinoma: excision removal | The two ellipses were joined into a long ellipse, and layered closure was done. 4-0 absorbable suture (Vicryl) was used for the deep dermals, and 4-0 monofilament (Prolene) was used for the superficial running suture. Note the eversion of the wound. | Surgical Methods | Knowledge Weavers Dermatology |
| 852 |
 |
Shave technique | The blade is held between the thumb and third finger using the index finger for curvature. Of course, gloves should always be used. The lesion should be shaved flush with the surrounding skin. | Shave Biopsy | Knowledge Weavers Dermatology |
| 853 |
 |
Instruments for skin lesion removal | The standard set of instruments that is necessary for removal of skin lesions. | Knowledge Weavers Dermatology | |
| 854 |
 |
Children with scabies | In children, they can have pruritic red papules distributed over most of the body. | Knowledge Weavers Dermatology | |
| 855 |
 |
Puncture wounds | As part of the debridement, the puncture wound should be flushed with generous amounts of sterile saline, and then a bulk dressing should be applied to absorb any drainage. | Knowledge Weavers Dermatology | |
| 856 |
 |
Urticaria wheal | The appearance of typical urticaria wheal. | Knowledge Weavers Dermatology | |
| 857 |
 |
Severe nodulocystic acne | Severe nodulocystic acne virtually always requires Accutane to bring and keep it under control. Theoretically, the previously shown regimen of using an oral antibiotic, a topical antibacterial, and a comedolytic (Retin-A) should be used first, but rarely is this successful. I trained in the pre-Accu... | Accutane | Knowledge Weavers Dermatology |
| 858 |
 |
Shave biopsy | If the skin eruption is vesicular, the shave or punch biopsy should be done of apparently normal skin that is next to the edge of the blister. The 4 mm diameter specimen can be cut in half, and half submitted for standard stains, and half submitted for immunofluorescent staining. | Shave Biopsy | Knowledge Weavers Dermatology |
| 859 |
 |
Undermining with scalpel | This demonstrates undermining with a scalpel just beneath the dermis. | Surgical Methods | Knowledge Weavers Dermatology |
| 860 |
 |
Comedo extraction | Using the Bezzant method of comedo extraction (picking), I recommend pinching the skin to stabilize it. | Comedo | Knowledge Weavers Dermatology |
| 861 |
 |
Children with scabies | A child with scabies showing pruritic red papules around the nipples and in the axillae. | Knowledge Weavers Dermatology | |
| 862 |
 |
Removal of dead epidermis and dermis | This shows the removal of the dead epidermis and dermis with the exposure of the yellow fat. | Knowledge Weavers Dermatology | |
| 863 |
 |
Fibrous septae | Fibrous septae connect the dermis to the underlying fascia, and these fibrous septaeoften have to be cut during surgery to free the wound edges in order to be able to pull the wound together and close it with suture. | Surgical Methods | Knowledge Weavers Dermatology |
| 864 |
 |
Comedonal acne | Comedonal acne: open and closed comedos can be seen on this patient's skin. | Knowledge Weavers Dermatology | |
| 865 |
 |
Exaggerated insect bite reaction | Exaggerated insect bite reaction | Knowledge Weavers Dermatology | |
| 866 |
 |
Treatment of comedonal acne | Retin-A 0.025% cream. It is recommended that a person wait 20 to 30 minutes after washing the face before applying Retin-A, but I find that it is very difficult for people to remember to do that, and it markedly reduces the compliance. I recommend that they simply apply the medication immediately af... | Retin-A | Knowledge Weavers Dermatology |
| 867 |
 |
Shave biopsy | Diagnosis of basal or squamous cell carcinoma can be achieved usually by using a shave biopsy. The double-edged blade is held between the thumb and third finger to ensure stability. | Shave Biopsy | Knowledge Weavers Dermatology |
| 868 |
 |
Inflamed bulbar conjunctivae secondary to rosacea | Inflamed bulbar conjunctivae secondary to rosacea. | Knowledge Weavers Dermatology | |
| 869 |
 |
Sebaceous hyperplasia | Sebaceous hyperplasia. The lesions are flesh-colored or slightly white or yellow, are round, and often have a central indentation. They can be destroyed with electrocautery or laser. | Knowledge Weavers Dermatology | |
| 870 |
 |
Puncture wounds | The wound should be opened so it can be visualized and explored, and blind probing such as shown here is discouraged. | Knowledge Weavers Dermatology | |
| 871 |
 |
Red papules and pustules | When there are more than about 10 red papules and pustules, then an oral antibiotic should be added to the topical comedolytic and antibacterial creams. | Anti-Bacterial Agents | Knowledge Weavers Dermatology |
| 872 |
 |
Basal cell carcinoma | Close-up of basal cell carcinoma on the left cheek presumably induced by radiation and/or sunlight. | Knowledge Weavers Dermatology | |
| 873 |
 |
Thermal burn | This patient received a thermal burn to the buttocks, and there was complete destruction of the skin and some of the underlying fat. This shows the exposed fat after I debrided the necrotic skin. Normal fat appears yellow. | Knowledge Weavers Dermatology | |
| 874 |
 |
Opening acne lesions | People who pick deeply with their fingernails damage the dermis significantly and can create scarring that clinically looks like depressed areas, such as in this patient, or can be elevated areas. | Knowledge Weavers Dermatology | |
| 875 |
 |
Treatment for rosacea | . . . to take 500 mg of tetracycline at night. | Knowledge Weavers Dermatology | |
| 876 |
 |
Severe acne vulgaris | Severe acne vulgaris involving the chest. | Knowledge Weavers Dermatology | |
| 877 |
 |
Comedo extraction | The third step in the Bezzant method is to push at the base of the comedo with the comedo extractor to expel the contents. | Comedo | Knowledge Weavers Dermatology |
| 878 |
 |
Lipoma and layered closure | This shows the lipoma and the results of the layered closure. This was located on the back. | Knowledge Weavers Dermatology | |
| 879 |
 |
Cleocin-T lotion and Retin-A | This patient with more than 10 red papules and pustules is using one of the two topical programs shown: 1) Program on the left is Cleocin-T lotion applied twice daily, and Retin-A 0.025% cream applied at night. 2) Program on the right is application of benzoyl peroxide 2.5% gel each morning, and Ret... | Knowledge Weavers Dermatology | |
| 880 |
 |
Children with scabies | Same child with scabies showing the lesions in the web spaces, around nipples, umbilicus, and suspected lesions should be scraped with a curette or a #15 scalpel blade, and mineral oil is applied first to ensure that the scale tends to adhere to the scraping instrument and is retrievable. At least 2... | Knowledge Weavers Dermatology | |
| 881 |
 |
Anaphylaxis and epinephrine | If the patient is on beta-blockers, generally epinephrine will not work in anaphylaxis. Glucagon can be administered in its place, and 1 mm of glucagon can be given subcutaneously irrespective of body size. Nausea is the major side effect. | Knowledge Weavers Dermatology | |
| 882 |
 |
Occlusion of the apocrine sweat glands | Cysts on the vulvae that are produced by occlusion of the apocrine sweat glands. | Knowledge Weavers Dermatology | |
| 883 |
 |
Punch biopsy | I stabilize the skin with my non-dominant (left) hand by stretching or pinching the skin, and then holding the punch at the top and spinning it very rapidly while applying moderate pressure I very quickly obtain full thickness skin biopsy. | Knowledge Weavers Dermatology | |
| 884 |
 |
Stasis dermatitis | The area should then be wrapped with the gauze that is impregnated with zinc oxide ointment. The wrap should be started just above the toes, and continue to just below the knee. | Knowledge Weavers Dermatology | |
| 885 |
 |
Excision: vertical mattress suture | This demonstrates placement of the vertical mattress suture that is used to close the upper layer of the dermis and the epidermis.The first pass the needle enters the right side of the wound about 2 mm from the wound, penetrates the full thickness of the dermis and exits 2 mm from the wound edge on... | Knowledge Weavers Dermatology | |
| 886 |
 |
Leg amputation wound | This is a breakdown of the wound in the leg amputation of an elderly woman who is diabetic. | Knowledge Weavers Dermatology | |
| 887 |
 |
Nummular dermatitis | Lesions of nummular dermatitis that are starting to coalesce. | Knowledge Weavers Dermatology | |
| 888 |
 |
Thickness biopsy | One of the typical lesions is anesthetized, and then a 4 mm diameter punch of the full thickness skin is done. The skin in most areas is 2 mm in depth, and 4 mm on the back. The wound is then closed with 4-0 monofilament suture using a vertical mattress closure, and one or two sutures are placed. | Knowledge Weavers Dermatology | |
| 889 |
 |
Papulopustular eruption | Close-up view of the papulopustular eruption on this pregnant patient. | Knowledge Weavers Dermatology | |
| 890 |
 |
Seborrheic dermatitis | Seborrheic dermatitis involving the scalp. | Knowledge Weavers Dermatology | |
| 891 |
 |
Eversion of a wound | This shows a top view of the same wound, and the marked eversion. The reason eversion is achieved is that the forces acting on the wound are downward (as the scar contracts), and laterally from the natural tension created by the surrounding skin. If one anticipates those forces by everting the wound... | Knowledge Weavers Dermatology | |
| 892 |
 |
Chigger mite bites | This is the back of the patient who was infested with chiggers. Treatment consists of any of the following:1) topical steroids applied twice daily.2) oral antihistamines.3) on prednisone, 1 mg/kg per day until the itching resolves. | Chiggers | Knowledge Weavers Dermatology |
| 893 |
 |
Anaphylaxis | If anaphylaxis or severe urticaria develops, one can use epinephrine 1:1,000, and the dose should be 0.01 cc's per kg injected into the subcutaneous fat, and that should be repeated every 10 to 15 minutes as necessary until the eruption is under control. | Knowledge Weavers Dermatology | |
| 894 |
 |
Stasis dermatitis | An elastic wrap is then applied on top of the gauze. The elastic wrap should be applied as tightly as the patient can stand around the foot and ankle, and the pressure is gradually reduced as the wrap is continued up to below the knee. | Knowledge Weavers Dermatology | |
| 895 |
 |
Ingrown nail | Small cotton-tip swabs saturated with pheno are used to destroy the nail matrix. Times of application range from 10 seconds to 3 minutes, depending on the author. | Knowledge Weavers Dermatology | |
| 896 |
 |
Severe nodulocystic acne | This patient has severe nodulocystic acne. Not only does he have acne, but the inflammatory damage to the dermis has induced elevated scars called keloids. These are permanent. This type of acne rarely responds to creams and oral antibiotics, but does respond well to oral Accutane. | Accutane | Knowledge Weavers Dermatology |
| 897 |
 |
Severe acne vulgaris | Severe acne vulgaris involving the back, and associated keloidal scarring. | Knowledge Weavers Dermatology | |
| 898 |
 |
Comedo extraction | The second step in the Bezzant method is to poke a hole in the top of the comedo or papulopustule with a small gauge needle, such as a 30 gauge. This provides an exit for the material so that it will eject from the skin and not be extruded into surrounding skin when pressure is applied at the sides. | Comedo | Knowledge Weavers Dermatology |
| 899 |
 |
Opening comedos | The second step in opening comedos with a comedo extractor is to push downward with the instrument. | Comedo | Knowledge Weavers Dermatology |
| 900 |
 |
Treatment for rosacea | The alternative to tetracycline is minocycline, 100 mg twice daily, and it has the advantage that it can be taken with food, including dairy products, and rarely causes photosensitization. The disadvantage is that it is much more expensive than tetracycline, and it currently costs about $1.00 to $3.... | Knowledge Weavers Dermatology |