The Health Education Assets Library (HEAL) is a collection of over 22,000 freely available digital materials for health sciences education. The collection is now housed at the University of Utah J. Willard Marriott Digital Library.
TO
Filters: Collection: "ehsl_heal"
| Title | Description | Subject | Collection | ||
|---|---|---|---|---|---|
| 1001 |
 |
Scabies, diagnosis | This demonstrates the application of mineral oil to suspected scabies lesions prior to scraping. | Knowledge Weavers Dermatology | |
| 1002 |
 |
Seborrheic dermatitis | Seborrheic dermatitis involving the chest and armpits. | Knowledge Weavers Dermatology | |
| 1003 |
 |
Stratum corneum | The stratum corneum, the barrier layer, is very thin, and can be removed with scotch tape and by applying scotch tape to the skin repeatedly for 15 or 20 times. Even though it is physically thin it is a very resilient and effective barrier layer. | Stratum Corneum | Knowledge Weavers Dermatology |
| 1004 |
 |
Milium near the medial canthus of the right eye | Milium near the medial canthus of the right eye. | Knowledge Weavers Dermatology | |
| 1005 |
 |
Body lice | Body lice often are located in the seams of the clothing. The treatment is simply physically washing the lice off the body, and destroying them within the clothing by washing them in hot water or dry-cleaning them. Itching can be relieved with the use of topical steroids, oral antihistamines, or ora... | Knowledge Weavers Dermatology | |
| 1006 |
 |
Punch biopsy | This demonstrates anesthetizing the skin before doing a punch biopsy. The target is the epidermis and dermis, and the upper portion of the fat, and all those areas should be injected with local anesthetic. | Knowledge Weavers Dermatology | |
| 1007 |
 |
Basal cell carcinoma: excision removal | A layered closure was done using 4-0 absorbable suture as a deep dermal suture, and 4-0 nonabsorbable monofilament suture in a running pattern. Note the wound eversion. | Surgical Methods | Knowledge Weavers Dermatology |
| 1008 |
 |
Children with scabies | At least 20 red papules are scraped with a #15 blade or a curette. | Knowledge Weavers Dermatology | |
| 1009 |
 |
Recessive epidermolysis bullosa | Same child with recessive epidermolysis bullosa. The slightest abrasion on the skin would tear the epidermis from the underlying dermis, and this was true of the mucosa as well. The child had broad areas of dermis that were exposed, and the child was treated as a burn victim with Silvadene cream and... | Knowledge Weavers Dermatology | |
| 1010 |
 |
Benign nevus in a child | Benign nevus in a child. It has been found that if a nevus grows rapidly in a child that this is the most common indicator of melanoma, and is more important than the usual criteria of mixture of colors and/or jagged border. | Knowledge Weavers Dermatology | |
| 1011 |
 |
Pustules in scalp | Pustules in scalp. There is a type of folliculitis or, some say, a form of acne vulgaris that presents as red papules and pustules in the scalp. Regardless, this generally responds to tetracycline, 500 mg twice daily, or minocycline, 100 mg twice daily. | Knowledge Weavers Dermatology | |
| 1012 |
 |
Excision: suturing vertical mattress | When the long arm (needle bearing end) of the suture is held upward, it forms a natural V, and the needle holder is placed on the inside the long arm of the V. | Knowledge Weavers Dermatology | |
| 1013 |
 |
Ectodermal dysplasia | Ectodermal dysplasia on the vulvae. | Knowledge Weavers Dermatology | |
| 1014 |
 |
Scabies mite | Scabies mite | Knowledge Weavers Dermatology | |
| 1015 |
 |
Pubic lice | The patient often experiences itching throughout the groin area, and there are often numerous nits in the pubic hair. The lice can range from about the knees up to the eyelashes. It is important to examine the body hair to ensure that all areas that are infested are treated adequately. | Knowledge Weavers Dermatology | |
| 1016 |
 |
Skin tags | Skin tags can be snipped off with scissors. | Knowledge Weavers Dermatology | |
| 1017 |
 |
Phototoxic eruption in a patient using tetracycline | Phototoxic eruption in a patient using tetracycline. | Phototoxic | Knowledge Weavers Dermatology |
| 1018 |
 |
Oral antibiotic | If a patient has more than 15 red papules and pustules in association with the comedos, then usually an oral antibiotic is required in addition to the previously shown therapy (see Slide 37), and I generally use tetracycline, 500 mg tid, or minocycline, 100 mg bid as the oral antibiotic choice. | Knowledge Weavers Dermatology | |
| 1019 |
 |
Moderate papulopustular acne | Same patient as shown in 64 with moderate papulopustular acne. | Knowledge Weavers Dermatology | |
| 1020 |
 |
Ingrown nail | A broad band tourniquet is applied to the digit. | Knowledge Weavers Dermatology | |
| 1021 |
 |
Excising with scalpel | A partial or full thickness cut is made, and the blade should be kept perpendicular to the skin or angled outward. | Surgical Methods | Knowledge Weavers Dermatology |
| 1022 |
 |
Seborrheic dermatitis | Seborrheic dermatitis involving the scalp; for whatever reason the patient shaved his scalp. | Knowledge Weavers Dermatology | |
| 1023 |
 |
Specimen removal | The specimen of skin that is removed should be the same thickness throughout so that there is not an uneven appearance of the skin when the skin is closed with suture. | Knowledge Weavers Dermatology | |
| 1024 |
 |
Chigger mite bites | This patient was thought to be infested with chiggers and had exaggerated insect bite reaction. | Chiggers | Knowledge Weavers Dermatology |
| 1025 |
 |
Papulopustular flare of acne vulgaris | Close-up of the papulopustular flare of acne vulgaris in this patient. | Knowledge Weavers Dermatology | |
| 1026 |
 |
Necrotic tissue in ulcer | If an ulcer has any necrotic tissue, it then has to be removed. The necrotic tissue simply provides potential nutrition for the bacteria, and is of no benefit to the healing process. I found that ulcers on the malleoli are very sensitive and the slightest touching or movement induces significant pai... | Knowledge Weavers Dermatology | |
| 1027 |
 |
Trendelenburg position | In anaphylaxis the patient should be placed in the head down (Trendelenburg) position. | Knowledge Weavers Dermatology | |
| 1028 |
 |
Opening acne lesions | This summarizes the Bezzant method of picking. My experience with trying to tell people not to pick is that it doesn't work. I, therefore, teach them this method of opening acne lesions as it seems to cause much less trauma and has less potential for scarring than picking with fingernails or with ho... | Knowledge Weavers Dermatology | |
| 1029 |
 |
Puncture wounds | Puncture wounds, such as the one shown here in the hand should be anesthetized with lidocaine or lidocaine and bupivacaine without epinephrine. Epinephrine will further decrease oxygenation of the tissue and potentially facilitate the growth of anaerobic bacteria. | Knowledge Weavers Dermatology | |
| 1030 |
 |
Hyfrecator: burning skin lesions | When using the hyfrecator one should ensure that it is plugged into low, and for small growths a setting of 30 (3 watts) is used, and on larger growths a setting of 50 (5 watts) is used. | Hyfrecator | Knowledge Weavers Dermatology |
| 1031 |
 |
Head lice | Infestation with head lice at the nape of the neck produces redness and scaling of the skin, and the black/brown/gray nits (eggs) can be seen on the hair shafts, and occasionally the adult lice can be seen on the skin. | Knowledge Weavers Dermatology | |
| 1032 |
 |
Pemphigus vulgaris on the trunk | Pemphigus vulgaris on the trunk. | Knowledge Weavers Dermatology | |
| 1033 |
 |
Striae formation in the groin | Striae formation in the groin secondary to the use of topical steroids. Striae formation, often calledfracturesof the skin, are currently considered irreversible. | Striae | Knowledge Weavers Dermatology |
| 1034 |
 |
Atopic dermatitis involving the eyelids | Atopic dermatitis involving the eyelids. | Knowledge Weavers Dermatology | |
| 1035 |
 |
Basal cell carcinoma: excision removal | This gentleman had two basal cell carcinomas. | Surgical Methods | Knowledge Weavers Dermatology |
| 1036 |
 |
Radiation therapy for acne vulgaris | This patient had radiation therapy for her acne vulgaris, and has a scar demonstrating previous thyroidectomy for thyroid cancer presumably induced by the radiation, and has developed a basal cell carcinoma on her left cheek. | Knowledge Weavers Dermatology | |
| 1037 |
 |
Leg measurement | This demonstrates measurement of the leg before custom support hose is made. | Knowledge Weavers Dermatology | |
| 1038 |
 |
Nasal mask | Nasal mask, in a variety of sizes for adults and children. | Knowledge Weavers Dermatology | |
| 1039 |
 |
Exaggerated insect bite reaction | Exaggerated insect bite reaction. | Knowledge Weavers Dermatology | |
| 1040 |
 |
Lichen simplex chronicus | After repeated scratching, the epidermis thickens and darkens as shown here; this is called lichenification. | Knowledge Weavers Dermatology | |
| 1041 |
 |
Occlusion of blood flow to the skin | Occlusion of blood flow to the skin, either from internal vessel damage or from external pressure, an ulcer can be created. | Skin blood supply | Knowledge Weavers Dermatology |
| 1042 |
 |
Mild inflammatory acne | When a patient has comedos and associated red papules and/or pustules, a topical antibacterial is required. | Anti-Bacterial Agents | Knowledge Weavers Dermatology |
| 1043 |
 |
Topical acne therapy | The first few weeks of topical acne therapy can be accompanied by redness and flaking of the skin. Lubricants will help to control scaling, and if necessary, one can add 1% hydrocortisone lotion or cream twice daily to help to reduce the inflammation. | Drug Effects | Knowledge Weavers Dermatology |
| 1044 |
 |
Atopic dermatitis in children | Atopic dermatitis in children often manifests ascradle cap. This is redness and scaling involving the scalp, and can be the lone manifestation of this problem. | Knowledge Weavers Dermatology | |
| 1045 |
 |
Head lice | Infestation with head lice. Generally, there is dermatitis at the nape of the neck, and the itching tends to be accentuated there. | Knowledge Weavers Dermatology | |
| 1046 |
 |
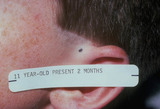
Halogenated steroids | Halogenated steroids, particularly fluorinated steroids, applied to the facial skin for over several weeks will often induce a dermatitis around the mouth, nose, and lower eyelids; this is called periorificial dermatitis. This inflammation usually, but not always, resolves spontaneously within seve... | Knowledge Weavers Dermatology | |
| 1047 |
 |
Eversion of a wound | This demonstrates eversion of the wound on the trunk created by a deep dermal suture. Often 3-0 absorbable suture has to be used on the trunk so that the suture does not break when it is being tied. | Knowledge Weavers Dermatology | |
| 1048 |
 |
Body louse | This is a body louse on the clothing of the same patient shown in 81. | Knowledge Weavers Dermatology | |
| 1049 |
 |
Basal cell carcinoma | Basal cell carcinoma. This patient had spent her younger years in Chihuahua, Mexico, and had been exposed to a lot of sunlight as a young person. This basal cell carcinoma originated within the epidermis and extended through the skin fat, and attached to the underlying muscle. | Knowledge Weavers Dermatology | |
| 1050 |
 |
Stasis dermatitis | If the patient has acute stasis dermatitis, then an Unna boot can be applied. This consists of a roll of gauze that is saturated with zinc oxide ointment, and an elastic wrap that is applied on top of it. | Knowledge Weavers Dermatology | |
| 1051 |
 |
Ectodermal dysplasia | Ectodermal dysplasia in the axillae. The patient also had abnormal nail plates and teeth. | Knowledge Weavers Dermatology | |
| 1052 |
 |
Undermining with scissors | This demonstrates undermining with scissors. The closed jaws are inserted beneath the dermis, and | Knowledge Weavers Dermatology | |
| 1053 |
 |
Thickness biopsy | When a patient has an eruption and the diagnosis is unknown, it is best to do a full thickness biopsy by doing a punch or small excision of one of the lesions. | Knowledge Weavers Dermatology | |
| 1054 |
 |
Seborrheic keratoses | Seborrheic keratoses. They are a benign thickening and darkening of the epidermis with varying amounts of loose adherent scale. | Knowledge Weavers Dermatology | |
| 1055 |
 |
Papulopustular eruption | Close-up view of the papulopustular eruption on this pregnant patient. | Knowledge Weavers Dermatology | |
| 1056 |
 |
Layered closure | Large lesions can be removed using the layered closure. This was a large lipoma on the back of a patient, and I removed this in my office. | Knowledge Weavers Dermatology | |
| 1057 |
 |
Children with scabies | Children who have scabies generally have inflammatory lesions in the axillae. This shows typical axillary lesions. | Knowledge Weavers Dermatology | |
| 1058 |
 |
Pregnant patient with papulopustular flare of acne vulgaris | Pregnant patient with papulopustular flare of acne vulgaris. To our knowledge, oral erythromycin or ampicillin or amoxicillin can be used safely, and topical erythromycin, clindamycin, or benzoyl peroxide also appear to be safe. | Knowledge Weavers Dermatology | |
| 1059 |
 |
Skin Tumor | Tumors of various sorts can be produced by anything that grows within the dermis.This demonstrates that the tumor was within the skin, and moves freely with the skin. | Knowledge Weavers Dermatology | |
| 1060 |
 |
Treatment of comedonal acne | When a patient has comedos along with less than about 15 red papules and pustules, one can use the regimen shown either on the patient's left or the patient's right. The method I usually use is shown on the patient's right: The patient is to apply benzoyl peroxide 2.5% gel to the face q am, and Reti... | Knowledge Weavers Dermatology | |
| 1061 |
 |
Venous pressure | With increased venous pressure induced by incompetent valves within the venous system of the leg, there is extravasation of fluid from the capillaries into the surrounding tissue. This separates the capillaries from the cells to which they supply nutrition, and those cells are damaged or even die. T... | Knowledge Weavers Dermatology | |
| 1062 |
 |
Ingrown nail | Appearance of ingrown nail. The nail plate is dystrophic, and in this case has induced significant foreign body reaction and secondary infection. | Knowledge Weavers Dermatology | |
| 1063 |
 |
Severe nodulocystic acne | This is the back of the same patient shown in Slide 16, and the nodules, cysts, and scarring are evident. This is both painful and disfiguring, and can have a profound detrimental psychological effect on the person who suffers this. Thankfully, we do have effective therapy now for it. | Knowledge Weavers Dermatology | |
| 1064 |
 |
Children with scabies | Child with scabies showing pruritic red papules around the ankle. | Knowledge Weavers Dermatology | |
| 1065 |
 |
Severe acne vulgaris | Severe acne vulgaris involving the back. | Knowledge Weavers Dermatology | |
| 1066 |
 |
Exaggerated insect bite reaction | Exaggerated insect bite reaction. | Knowledge Weavers Dermatology | |
| 1067 |
 |
Excision: suturing | The second throw is initiated by placing the needle holder on the inside the long arm (needle bearing end) of the V. | Knowledge Weavers Dermatology | |
| 1068 |
 |
Atopic dermatitis involving the perianal area | Atopic dermatitis involving the perianal area. | Knowledge Weavers Dermatology | |
| 1069 |
 |
Freezing with liquid nitrogen | Freezing is done to mainly destroy epidermal growths. As long as the indicated freezing times are followed, generally there is no scarring. Occasionally the dermis is injured as shown here, and hypertrophic or keloid scars can be formed, especially on areas of tension, such as the elbow. | Knowledge Weavers Dermatology | |
| 1070 |
 |
Excision: knot tying | The needle holder is placed on the inside the long arm (needle bearing end) of the V as shown. Before beginning to tie the knot, insure that the two ends of the suture come out the same side of the loop, and that the order is: loop, short (non-needle bearing) end, long (needle bearing) end. | Knowledge Weavers Dermatology | |
| 1071 |
 |
Recessive epidermolysis bullosa | This child has recessive epidermolysis bullosa. | Knowledge Weavers Dermatology | |
| 1072 |
 |
Treatment for rosacea | Typical treatment for rosacea is to take 500 mg of tetracycline in the morning, and . . . | Knowledge Weavers Dermatology | |
| 1073 |
 |
Normal fat at the base of a debrided wound of the heel | This shows normal fat, but note is bleeding freely. I found when debriding a wound it is best to give an oral or injected analgesic before debridement, and when the patient is quite relaxed I then infuse the area to be debrided with a mixture of lidocaine and bupivacaine with epinephrine. | Surgical Methods | Knowledge Weavers Dermatology |
| 1074 |
 |
Punch biopsy | The plug should be gently lifted with forceps, and the fatty strand at the base should be snipped. | Knowledge Weavers Dermatology | |
| 1075 |
 |
Stasis dermatitis | The area should be first cleansed with sterile saline or soap and water. | Knowledge Weavers Dermatology | |
| 1076 |
 |
Nummular dermatitis | Lesions of acute (red and oozing) nummular dermatitis on the trunk. | Knowledge Weavers Dermatology | |
| 1077 |
 |
Atopic dermatitis in children | Atopic dermatitis often involves the cheeks of children. | Knowledge Weavers Dermatology | |
| 1078 |
 |
Incompetent venous system of the legs | The next step in damage to the skin from an incompetent venous system of the legs is lipo dermatosclerosis. In this condition, there is an increased amount of fibrous tissue both within the dermis and the underlying fat. The extremities appear tense and shiny, and they feel woody and hard to the tou... | Knowledge Weavers Dermatology | |
| 1079 |
 |
Scabies with inflamed lesions in a paraumbilical distribution | Same nursing home patient with scabies with inflamed lesions in a paraumbilical distribution. | Knowledge Weavers Dermatology | |
| 1080 |
 |
Milium extraction | The appearance after extraction of the milium. | Knowledge Weavers Dermatology | |
| 1081 |
 |
Ingrown nail | After cleaning the blood from the toe with hydrogen peroxide and removing the tourniquet, I apply a bulky dressing to absorb the blood, as it may bleed for up to about an hour if the foot is dependent. | Knowledge Weavers Dermatology | |
| 1082 |
 |
Insect Bites | Itchy insect bites can be treated with a topical steroid; I prefer to use an ultra-potent topical steroid, such as Temovate, twice daily to the inflamed lesions. | Knowledge Weavers Dermatology | |
| 1083 |
 |
Undermining with scalpel | This demonstrates undermining of the dermis using a scalpel. | Knowledge Weavers Dermatology | |
| 1084 |
 |
Scabies with flexural wrist involvement | Same patient with flexural wrist involvement. In this scenario, not only should the patient be treated, but all family members who have had skin-to-skin contact with the patient, as well as nursing personnel and housekeeping personnel who have had contact with the patient. | Knowledge Weavers Dermatology | |
| 1085 |
 |
Recessive epidermolysis bullosa | A baby with recessive epidermolysis bullosa. This patient links adequate numbers of anchoring fibrils (collagen type 7) to attach epidermis to the underlying dermis. | Knowledge Weavers Dermatology | |
| 1086 |
 |
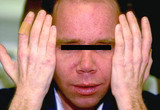
Atrophy of facial skin | Atrophy of facial skin induced by overuse of topical steroids to facial skin. The vessels of the deeper dermis and fat can be seen through the thin epidermis/dermis. Upon cessation of use of the steroids, the skin should regain its normal thickness, but it takes months to years for that to occur in ... | Adverse Effects | Knowledge Weavers Dermatology |
| 1087 |
 |
Acne surgery | The person appears blotchy immediately after acne surgery, and it takes one to two days for that to resolve. I always ask the patient about upcoming social events or photo sessions over the next several days before initiating acne surgery. | Surgical Methods | Knowledge Weavers Dermatology |
| 1088 |
 |
Atopic dermatitis involving the neck | Atopic dermatitis involving the neck. | Knowledge Weavers Dermatology | |
| 1089 |
 |
Anaphylactic shock | During anaphylactic shock, blood pressure should be monitored regularly. | Knowledge Weavers Dermatology | |
| 1090 |
 |
Acute stasis dermatitis | Acute stasis dermatitis, manifested as redness and oozing. | Knowledge Weavers Dermatology | |
| 1091 |
 |
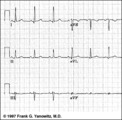
LVH - best seen in the frontal plane leads! | LVH - best seen in the frontal plane leads! | Knowledge Weavers ECG | |
| 1092 |
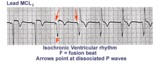 |
Isochronic ventricular rhythm | An isochronic ventricular rhythm is also called an accelerated ventricular rhythm because it represents an active ventricular focus. This arrhythmia is a common reperfusion arrhythmia in acute MI patients. It often begins and ends with fusion beats and there is AV dissociation. Treatment is usuall... | Knowledge Weavers ECG | |
| 1093 |
 |
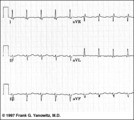
LVH: limb lead criteria | In this example of LVH, the precordial leads don't meet the usual voltage criteria or exhibit significant ST segment abnormalities. The frontal plane leads, however, show voltage criteria for LVH and significant ST segment depression in leads with tall R waves. The voltage criteria include 1) R in... | Knowledge Weavers ECG | |
| 1094 |
 |
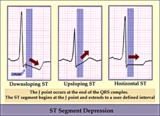
ST segment depression | ST segment depression is a nonspecific abnormality that must be evaluated in the clinical context in which it occurs. In a patient with angina pectoris ST depression usually means subendocardial ischemia and, unlike ST elevation, is not localizing to a particular coronary artery lesion. | Knowledge Weavers ECG | |
| 1095 |
 |
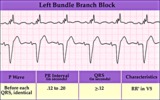
Rate-dependent LBBB | In this rhythm strip of sinus arrhythmia, the faster rates have a LBBB morphology. In some patients with a diseased left bundle branch, the onset of LBBB usually occurs initially as a rate-dependent block; i.e., the left bundle fails to conduct at the faster rate because of prolonged refractoriness... | Knowledge Weavers ECG | |
| 1096 |
 |
RV vs LV PVC's - marquette | RV vs LV PVC's - marquette | Knowledge Weavers ECG | |
| 1097 |
 |
RBBB: Precordial leads | RBBB: Precordial leads | Knowledge Weavers ECG | |
| 1098 |
 |
Inferior MI and RBBB | Inferior MI and RBBB | Knowledge Weavers ECG | |
| 1099 |
 |
Atrial parasystole | Parasystolic rhythms involve an independent ectopic pacemaker resulting in nonfixed coupled premature beats. Parasystole may occur in the atria, as seen in this example, in the AV junction, and in the ventricles. Note the common inter-ectopic interval separating the parasystolic PAC's. | Knowledge Weavers ECG | |
| 1100 |
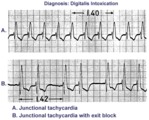 |
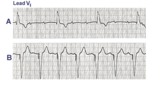
Digitalis intoxication: junctional tachycardia with and without exit block | In A the rhythm is junctional tachycardia with RBBB. In B there is 2nd degree exit block with a 3:2 conduction ratio; i.e., every 3rd junctional impulse fails to reach the ventricles... at least for the first two groupings on 1.4sec. | Knowledge Weavers ECG | |
| 1101 |
 |
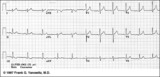
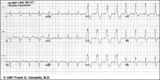
LVH and many PVCs | The combination of voltage criteria (SV2 + RV6>35mm) and ST-T abnormalities in V5-6 are definitive for LVH. There may also be LAE as evidenced by the prominent negative P terminal force in lead V1. Isolated PVCs and a PVC couplet are also present. | Knowledge Weavers ECG | |
| 1102 |
 |
Frontal plane QRS axis = +150 degrees (RAD) | This is an unusual right axis deviation (RAD). Lead I is negative, which usually means RAD. Lead II is the isoelectric lead, which almost always means -30 degrees; but in this example the axis is 180 degrees away from -30, or +150 degrees. | Knowledge Weavers ECG | |
| 1103 |
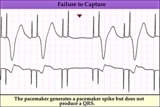 |
Pacemaker failure to capture - marquette | Pacemaker failure to capture - marquette | Knowledge Weavers ECG | |
| 1104 |
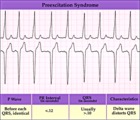 |
WPW type preexcitation - marquette | WPW type preexcitation - marquette | Knowledge Weavers ECG | |
| 1105 |
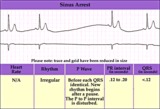 |
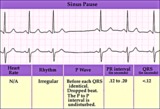
Sinus pause or arrest - marquette | Sinus pause or arrest - marquette | Knowledge Weavers ECG | |
| 1106 |
 |
SA exit block - marquette | SA exit block - marquette | Knowledge Weavers ECG | |
| 1107 |
 |
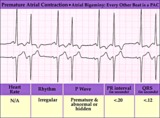
An interpolated PAC | Although most PACs reset the sinus node producing an incomplete compensatory pause, this PAC, indicated by the black arrow, is interpolated, i.e., sandwiched between two sinus beats. Note that the subsequent sinus P wave conducts with prolonged PR interval due to the relative refractoriness of the... | Knowledge Weavers ECG | |
| 1108 |
 |
Incomplete AV dissociation due To 2nd degree AV block | 2nd degree AV block is evident from the nonconducted P waves. Junctional escapes, labled J, terminate the long pauses because that's the purpose of escape pacemakers....to protect us from too slow heart rates. All QRSs with shorter RR intervals are capture beats, labeled c. Atypical RBBB with a q... | Knowledge Weavers ECG | |
| 1109 |
 |
Frontal plane QRS axis = +50 degrees | 1) lead aVL is the smallest QRS and closest to being the isoelectric lead; 2) perpendiculars to aVL are +60 and -120 degrees; 3) lead I is positive; 4) therefore, the axis is closest to being +60 degrees. Because aVL is actually slightly positive, the axis is only about +50 degrees (i.e., slightly ... | Knowledge Weavers ECG | |
| 1110 |
 |
Atypical LBBB with primary T wave abnormalities | Primary T wave abnormalities in LBBB refer to T waves in the same direction as the major deflection of the QRS. These are seen in leads I, III, aVL, V2-4. Most likely diagnosis is myocardial infarction. | Knowledge Weavers ECG | |
| 1111 |
 |
Mobitz II 2nd degree AV block with LBBB | The QRS morphology in lead V1 shows LBBB. The arrows point to two consecutive nonconducted P waves, most likely hung up in the diseased right bundle branch. This is classic Mobitz II 2nd degree AV block. | Knowledge Weavers ECG | |
| 1112 |
 |
RBBB with primary ST-T abnormalities: Precordial leads | RBBB with primary ST-T abnormalities: Precordial leads | Knowledge Weavers ECG | |
| 1113 |
 |
Bifascicular block: RBBB + LAFB | Bifascicular block: RBBB + LAFB | Knowledge Weavers ECG | |
| 1114 |
 |
PVC with R-on-T - marquette | PVC with R-on-T - marquette | Knowledge Weavers ECG | |
| 1115 |
 |
PVCs - marquette | PVCs - marquette | Knowledge Weavers ECG | |
| 1116 |
 |
Right Ventricular Hypertrophy (RVH) & Right Atrial Enlargement (RAE) | In this case of severe pulmonary hypertension, RVH is recognized by the prominent anterior forces (tall R waves in V1-2), right axis deviation (+110 degrees), and P pulmonale (i.e., right atrial enlargement). RAE is best seen in the frontal plane leads; the P waves in lead II are >2.5mm in amplitud... | Knowledge Weavers ECG | |
| 1117 |
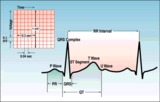 |
ECG intervals and waves | The P wave represents atrial activation; the PR interval is the time from onset of atrial activation to onset of ventricular activation. The QRS complex represents ventricular activation; the QRS duration is the duration of ventricular activation. The ST-T wave represents ventricular repolarizatio... | Knowledge Weavers ECG | |
| 1118 |
 |
Atrial flutter with 2:1 AV conduction | Flutter waves are best seen in lead V1; one immediately follows the QRS and the other precedes the next QRS. The regular ventricular rate of 150 bpm should always prompt us to condider this diagnosis. | Knowledge Weavers ECG | |
| 1119 |
 |
Left axis deviation: QRS axis = -45 degrees | There is no isoelectric, but leads aVR and II are the closest to being isoelectric, placing the axis between -30 and -60 degrees. The axis, therefore, is about -45 degrees. | Knowledge Weavers ECG | |
| 1120 |
 |
Long QT: an ECG marker for sudden cardiac death | Long QT: an ECG marker for sudden cardiac death | Knowledge Weavers ECG | |
| 1121 |
 |
Frontal plane QRS axis = 0 degrees | Frontal plane QRS axis = 0 degrees | Knowledge Weavers ECG | |
| 1122 |
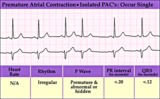 |
Isolated PAC - marquette | Isolated PAC - marquette | Knowledge Weavers ECG | |
| 1123 |
 |
Inferolateral ST segment elevation | ST Segment elevation with a straight or convex upwards configuration usually means transmural ischemia (or injury) and is seen in the setting of acute myocardial infarction. This ECG finding may also be seen transiently during coronary artery spasm. Unlike ST depression, ST elevation is often loca... | Knowledge Weavers ECG | |
| 1124 |
 |
A PAC initiates paroxysmal atrial fibrillation | The arrow indicates slight alteration of the ST-T wave by a PAC. The PAC, in turn, falls during the vulnerable period of atrial repolarization and initiates atrial fibrillation. Similar but more catastrophic events happen in the ventricles when PVC's occur during the vulnerable period, i.e. R-on-T... | Knowledge Weavers ECG | |
| 1125 |
 |
Left Atrial Abnormality & 1st Degree AV Block | The P-wave is notched, wider than 0.12s, and has a prominent negative (posterior) component in V1 - all criteria for left atrial abnormality or enlargement (LAE). The PR interval >0.20s. Minor ST-T wave abnormalities are also present. | Knowledge Weavers ECG | |
| 1126 |
 |
3rd degree AV block rx'ed with a ventricular pacemaker | In A the ECG shows complete or 3rd degree AV block with a left ventricular escape rhythm, as evidenced by the upright QRS morphology. In B the artificial right ventricular pacemaker rhythm is shown. | Knowledge Weavers ECG | |
| 1127 |
 |
Lead Error: V1 & V3 are Transposed | In this normal 12-lead ECG the V1 and V3 chest electrodes are interchanged. Experienced ECG interpreters should be able to spot this lead placement error. | Knowledge Weavers ECG | |
| 1128 |
 |
PAC and PVC: complete vs. incomplete pause | PAC and PVC: complete vs. incomplete pause | Knowledge Weavers ECG | |
| 1129 |
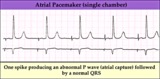 |
Electronic atrial pacing - marquette | Electronic atrial pacing - marquette | Knowledge Weavers ECG | |
| 1130 |
 |
Normal sinus rhythm - marquette | Normal sinus rhythm - marquette | Knowledge Weavers ECG | |
| 1131 |
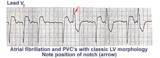 |
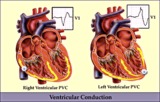
Left ventricular PVC's | In lead V1, these PVC's are positive or anterior in direction indicating probable LV origin with late activation of the right ventricle. The arrow points to the notch on the downstroke of the PVC making its morphology highly unlikely to be an aberrantly conducted supraventricular beat. | Knowledge Weavers ECG | |
| 1132 |
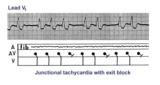 |
Junctional tachycardia with exit block: a manifestation of digitalis intoxication | Theladder diagramsays it all: the atria are fibrillating; there is complete heart block in the AV junction; a junctional tachycardia focus is firing at about 130 bpm, but not all junctional impulses reach the ventricles due to 2nd degree exit block. | Knowledge Weavers ECG | |
| 1133 |
 |
Frontal plane QRS axis = +90 degrees | 1) Lead I is isoelectric; 2) perpendiculars to lead I are +90 and -90 degrees; 3) leads II, III, aVF are positive; 4) therefore, the axis must be +90 degrees. | Knowledge Weavers ECG | |
| 1134 |
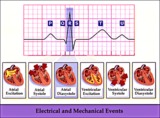 |
Electrical and mechanical events diagram - marquette | Electrical and mechanical events diagram - marquette | Knowledge Weavers ECG | |
| 1135 |
 |
Anteroseptal MI, fully evolved: precordial leads | Anteroseptal MI, fully evolved: precordial leads | Knowledge Weavers ECG | |
| 1136 |
 |
Left atrial enlargement: leads II and V1 | Left atrial enlargement: leads II and V1 | Knowledge Weavers ECG | |
| 1137 |
 |
Fully evolved inferior MI: frontal plane | Fully evolved inferior MI: frontal plane | Knowledge Weavers ECG | |
| 1138 |
 |
Frontal plane QRS axis = -75 degrees | Frontal plane QRS axis = -75 degrees | Knowledge Weavers ECG | |
| 1139 |
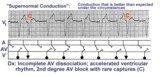 |
Supernormal conduction: 2nd degree AV block with rare captures; accelerated ventricular rhythm | This complicated rhythm strip illustrates 'supernormal' conduction... a situation where conduction is better than expected. The ladder diagram shows that the accelerated ventricular rhythm prevents most of the sinus impulses from reaching the ventricles. Only appropriately timed sinus impulses rea... | Knowledge Weavers ECG | |
| 1140 |
 |
Complete AV block, junctional escape rhythm, and ventriculophasic sinus arrhythmia | Complete AV block is seen as evidenced by the AV dissociation. A junctional escape rhythm sets the ventricular rate at 45 bpm. The PP intervals vary because of ventriculophasic sinus arrhythmia; this is defined when the PP interval that includes a QRS is shorter than a PP interval that excludes a ... | Knowledge Weavers ECG | |
| 1141 |
 |
Junctional parasystole and pseudo-AV block | This complicated rhythm strip shows normal sinus rhythm and a competing junctional parasystolic focus. Solid circles indicate junctional premature beats from the parasystolic focus. Open circles indicate non-conducted junctional prematures; the first open circle is a nonconducted junctional prematur... | Knowledge Weavers ECG | |
| 1142 |
 |
Premature junctional complexes with retrograde P waves | The ladder diagram illustrates the PJC with retrograde atrial capture | Knowledge Weavers ECG | |
| 1143 |
 |
Left Atrial Abnormality & 1st Degree AV Block: Leads II and V1 | Left Atrial Abnormality & 1st Degree AV Block: Leads II and V1 | Knowledge Weavers ECG | |
| 1144 |
 |
Right Axis Deviation & RAE (P pulmonale): Leads I, II, III | Right Axis Deviation & RAE (P pulmonale): Leads I, II, III | Knowledge Weavers ECG | |
| 1145 |
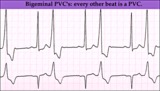 |
Ventricular bigeminy - marquette | Ventricular bigeminy - marquette | Knowledge Weavers ECG | |
| 1146 |
 |
LBBB and 2nd degree AV block, mobitz type I | Mobitz II 2nd degree AV block is usually a sign of bilateral bundle branch disease. One of the two bundle branches should be completely blocked; in this example the left bundle is blocked. The nonconducted sinus P waves are most likely blocked in the right bundle which exhibits 2nd degree block. ... | Knowledge Weavers ECG | |
| 1147 |
 |
Infero-posterior MI&RBBB | Deep Q waves in II, III, aVF plus tall R waves in V1-2 are evidence for this infero-posterior MI. The wide QRS (>0.12s) and RR' complex in V1 are evidence for RBBB. Any time RBBB has an initial R in V1 equal to or greater than the R', true posterior MI must be considered. Q waves in V5-6 suggest a... | Knowledge Weavers ECG | |
| 1148 |
 |
Extensive anterior/anterolateral MI: recent | Significant pathologic Q-waves (V2-6, I, aVL) plus marked ST segment elevation are evidence for this large anterior/anterolateral MI. The exact age of the infarction cannot be determined without clinical correlation and previous ECGs, but this is likely a recent MI. | Knowledge Weavers ECG | |
| 1149 |
 |
Nonconducted PAC's slowing the heart rate | Consecutive nonconducted PAC's, indicated by arrows, can significantly slow the heart rate. Note the distortion of the ST-T waves caused by the PAC. A hint in recognizing nonconducted PAC's is to find conducted PAC's in the same rhythm strip. | Knowledge Weavers ECG | |
| 1150 |
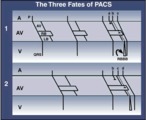 |
three fates of PAC's: 1. normal conduction; 2. aberrant conduction; 3. non-conduction | three fates of PAC's: 1. normal conduction; 2. aberrant conduction; 3. non-conduction | Knowledge Weavers ECG | |
| 1151 |
 |
QRS axis = 0 degrees | Lead aVF is isoelectric; lead I is positive; therefore, the QRS axis is 0 degrees. | Knowledge Weavers ECG | |
| 1152 |
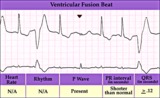 |
Ventricular fusion beat - marquette | Ventricular fusion beat - marquette | Knowledge Weavers ECG | |
| 1153 |
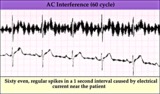 |
60 cycle artifact - marquette | 60 cycle artifact - marquette | Knowledge Weavers ECG | |
| 1154 |
 |
LBBB: precordial leads | LBBB: precordial leads | Knowledge Weavers ECG | |
| 1155 |
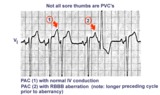 |
Not all sore thumbs are ventricular in origin | PACs have three fates: normal conduction into ventricles, aberrant conduction in ventricles due to bundle branch or fascicular block, and non-conduction due to block in AV junction. In this example PAC 1 is normally conducted and PAC 2 is conducted with RBBB aberration. The longer preceding cycle ... | Knowledge Weavers ECG | |
| 1156 |
 |
Acute infero-postero-lateral MI | Hyperacute ST segment elevation is seen in leads II, III, aVF (inferior location) and in leads V4-6 (apical lateral wall location). Hyperacute ST depression is seen in leads V1-2 (an expression of posterior wall injury). in addition there are reciprocal ST segment depression changes in leads I an... | Knowledge Weavers ECG | |
| 1157 |
 |
Ventricular Pacemaker Rhythm: V1-3 | Note the small pacemaker spikes before the QRS complexes. In addition, the QRS complex in V1-3 exhibits ventricular ectopic morphology; i.e., there is a slur or notch at the beginning of the S wave, and >60ms delay from onset to QRS to nadir of S wave. This rules against a supraventricular rhythm wi... | Knowledge Weavers ECG | |
| 1158 |
 |
Inferior MI: fully evolved | Significant pathologic Q-waves are seen in leads II, III, aVF along with resolving ST segment elevation and symmetrical T wave inversion. This is a classic inferior MI. | Knowledge Weavers ECG | |
| 1159 |
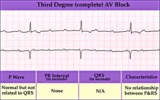 |
Complete AV block (3rd degree) with junctional rhythm | Complete AV block (3rd degree) with junctional rhythm | Knowledge Weavers ECG | |
| 1160 |
 |
QRS axis = +90 degrees | Lead I is isoelectric; II and III are positive; the axis is +90 degrees. | Knowledge Weavers ECG | |
| 1161 |
 |
Left bundle branch block - marquette | Left bundle branch block - marquette | Knowledge Weavers ECG | |
| 1162 |
 |
Junctional escape rhythm | Junctional escape rhythm | Knowledge Weavers ECG | |
| 1163 |
 |
Diagram: AV nodal reentrant tachycardia | The AV node often has dual pathways; in this diagram the alpha pathway is fast, but has a long refractory period; the beta pathway is conducts more slowly, but recovers faster.In sinus rhythm the faster alpha pathway is used and accounts for the normal PR interval. When a PAC occurs, however, the i... | Knowledge Weavers ECG | |
| 1164 |
 |
Atrial parasystole | In atrial parasystole non-fixed coupled PACs, shown by arrows, occur at a common inter-ectopic interval or at multiples of this interval. Atrial fusions, not shown here, may also occur when the PAC occurs in close temporal proximity to the sinus impulse. | Knowledge Weavers ECG | |
| 1165 |
 |
Atrial flutter with 2:1 conduction: leads II, III, V1 | Atrial flutter with 2:1 conduction: leads II, III, V1 | Knowledge Weavers ECG | |
| 1166 |
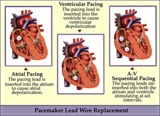 |
Pacemaker lead wire placement diagram - marquette | Pacemaker lead wire placement diagram - marquette | Knowledge Weavers ECG | |
| 1167 |
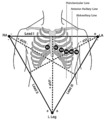 |
Frontal and horizontal plane lead diagram | Frontal and horizontal plane lead diagram | Knowledge Weavers ECG | |
| 1168 |
 |
ST segment diagram - marquette | ST segment diagram - marquette | Knowledge Weavers ECG | |
| 1169 |
 |
Atrial bigeminy - marquette | Atrial bigeminy - marquette | Knowledge Weavers ECG | |
| 1170 |
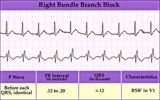 |
Right Bundle Branch Block | Right Bundle Branch Block | Knowledge Weavers ECG | |
| 1171 |
 |
2nd degree AV block, type I, with accelerated junctional escapes and a ladder diagram | The ladder diagram illustrates a Wenckebach type AV block by the increasing PR intervals before the blocked P wave. After the blocked P wave, however, a rev-ed up junctional pacemaker terminates the pause. Note that the junctional beats have a slightly different QRS morphology from the sinus beats... | Knowledge Weavers ECG | |
| 1172 |
 |
Atrial tachycardia with exit block and AV block | The ectopic P waves, easily seen in this example,occur in groups, separated by short pauses. This is likely due to an exit block just distal to the atrial pacemaker. Because not all of the P waves make it to the ventricles, there is also 2nd degree AV block. Therefore, two levels of block are pre... | Knowledge Weavers ECG | |
| 1173 |
 |
LVH | In this example of LVH, the precordial leads don't meet the usual voltage criteria or exhibit significant ST segment abnormalities. The frontal plane leads, however, show voltage criteria for LVH and significant ST segment depression in leads with tall R waves. The voltage criteria include 1) R in a... | Knowledge Weavers ECG | |
| 1174 |
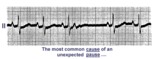 |
A nonconducted PAC causes an unexpected pause | Unexpected pauses in rhythm have several causes, the most frequent being a nonconducted PAC. In this example the nonconducted PAC is seen in the ST segment of the pause. Note the change in the ST-T compared to the other ST-T waves. | Knowledge Weavers ECG | |
| 1175 |
 |
Giant TU fusion waves | TU fusion waves are often seen in long QT syndromes. The differential diagnosis of this ECG abnormality includes electrolyte abnormalities -hypokalemia, CNS disease, e.g., subarachnoid hemorrhage; hereditary long QT syndromes, and drugs such as quinidine. | Knowledge Weavers ECG | |
| 1176 |
 |
Left anterior fascicular block (LAFB) | LAFB is the most common of the intraventricular conduction defects. It is recognized by 1) left axis deviation; 2) rS complexes in II, III, aVF; and 3) small q in I and/or aVL. | Knowledge Weavers ECG | |
| 1177 |
 |
Atrial flutter with 2:1 AV conduction: lead V1 | The arrows point to two flutter waves for each QRS complex. Atrial rate = 280; ventricular rate = 140. | Knowledge Weavers ECG | |
| 1178 |
 |
Long QT Interval and Giant Negative T Waves | Long QT Interval and Giant Negative T Waves | Knowledge Weavers ECG | |
| 1179 |
 |
Frontal plane QRS axis = -15 degrees | Frontal plane QRS axis = -15 degrees | Knowledge Weavers ECG | |
| 1180 |
 |
Ventricular pacemaker rhythm | Note the small pacemaker spikes before the QRS complexes in many of the leads. In addition, the QRS complex in V1 exhibits ventricular ectopic morphology; i.e., there is a slur or notch at the beginning of the S wave, and>60ms delay from onset to QRS to nadir of S wave. This rules against a suprav... | Knowledge Weavers ECG | |
| 1181 |
 |
Diffuse anterolateral T wave abnormalities | Diffuse anterolateral T wave abnormalities | T Wave Abnormalities | Knowledge Weavers ECG |
| 1182 |
 |
Frontal plane QRS axis = -45 degrees | Frontal plane QRS axis = -45 degrees | Knowledge Weavers ECG | |
| 1183 |
 |
Marked sinus arrhythmia - marquette | Marked sinus arrhythmia - marquette | Knowledge Weavers ECG | |
| 1184 |
 |
Muscle tremor artifact - marquette | Muscle tremor artifact - marquette | Knowledge Weavers ECG | |
| 1185 |
 |
RBBB + LAFB: bifascicular block | RBBB + LAFB: bifascicular block | Knowledge Weavers ECG | |
| 1186 |
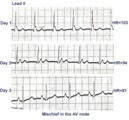 |
ECG of the century: A most unusual 1st degree AV block | On Day 1, at a heart rate of 103 bpm the P waves are not clearly defined suggesting an accelerated junctional rhythm. However, on Day 2, at a slightly slower heart rate the sinus P wave suddenly appears immediately after the QRS complex. In retrospect, the sinus P wave in Day 1 was found burried i... | Knowledge Weavers ECG | |
| 1187 |
 |
RBBB plus mobitz II 2nd degree AV block | The classic rSR' in V1 is RBBB. Mobitz II 2nd degree AV block is present because the PR intervals are constant. Statistically speaking, the location of the 2nd degree AV block is in the left bundle branch rather than in the AV junction. The last QRS in the top strip is a junctional escape, since... | Knowledge Weavers ECG | |
| 1188 |
 |
Left axis deviation: QRS axis = -60 degrees | Lead aVR is isoelectric; leads II and III are mostly negative. The QRS axis, therefore, is -60 degrees. | Knowledge Weavers ECG | |
| 1189 |
 |
QRS axis = +30 degrees | Lead III is isoelectric; leads I and II are positive. The QRS axis, therefore, is +30 degrees. | Knowledge Weavers ECG | |
| 1190 |
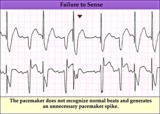 |
Pacemaker failure to sense - marquette | Pacemaker failure to sense - marquette | Knowledge Weavers ECG | |
| 1191 |
 |
Pacemaker fusion beat - marquette | Pacemaker fusion beat - marquette | Knowledge Weavers ECG | |
| 1192 |
 |
RAE & RVH | RAE & RVH | Knowledge Weavers ECG | |
| 1193 |
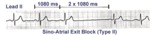 |
Type II, 2nd degree sino-atrial block | Two types of 2nd degree SA block have been described. In type-I, or SA Wenckebach, the P-P interval of the pause is less than 2x the preceding P-P intervals. In type-II SA block the P-P interval of the pause is approximately 2x the normal P-P interval. The distinction between types I and II is no... | Knowledge Weavers ECG | |
| 1194 |
 |
Bradycardia-dependent LBBB with carotid sinus massage | When carotid sinus massage slows the heart rate in this example, the QRS widens into a LBBB. This form of rate-dependent bundle branch block is thought to be due to latent pacemakers in the bundle undergoing phase 4 depolarization; when the sinus impulse enters the partially depolarized bundle, slow... | Knowledge Weavers ECG | |
| 1195 |
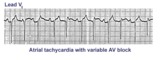 |
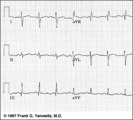
Atrial tachycardia with 3:2 AV block | In this rhythm the atrial rate from an ectopic focus is 160 bpm. Atrial activity can be seen on top of T waves, and before QRS's. Careful observation reveals a 3:2 Wenckebach relationship between P waves and QRS's. Atrial tachycardia with block is often a sign of digitalis intoxication. | Knowledge Weavers ECG | |
| 1196 |
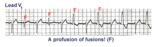 |
Ventricular fusion beats | Fusion beats occur when two or more activation fronts contribute to the electrical event. These may occur in the atria or in the ventricles. In this example the ventricular fusions are the result of simultaneous activation of the ventricles from two foci, the sinus node and a ventricular ectopic... | Knowledge Weavers ECG | |
| 1197 |
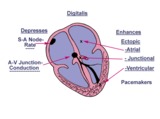 |
Diagram: digitalis effect on rhythm and conduction | Diagram: digitalis effect on rhythm and conduction | Knowledge Weavers ECG | |
| 1198 |
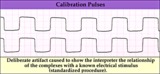 |
Calibration signal - marquette | Calibration signal - marquette | Knowledge Weavers ECG | |
| 1199 |
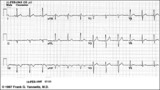 |
Old inferior MI | Old inferior MI | Knowledge Weavers ECG | |
| 1200 |
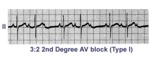 |
Second degree AV block, type I, with 3:2 conduction ratio | There are two types of 2nd degree AV Block. In this example of Type I or Wenckebach AV block there are 3 P waves for every 2 QRSs; the PR interval increases until a P wave fails to conduct. This is an example of group beating. | Knowledge Weavers ECG |