The Health Education Assets Library (HEAL) is a collection of over 22,000 freely available digital materials for health sciences education. The collection is now housed at the University of Utah J. Willard Marriott Digital Library.
TO
Filters: Collection: "ehsl_heal"
| Title | Description | Subject | Collection | ||
|---|---|---|---|---|---|
| 1201 |
 |
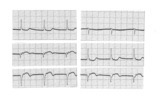
Infero-posterior MI with RBBB | This is an unusual RBBB because the initial R wave is taller than the R wave in lead V1. This is the clue for true posterior MI. The tall initial R wave in V1 is a pathologic R wave analagous to the pathologic Q wave of an anterior MI. | Knowledge Weavers ECG | |
| 1202 |
 |
Right Atrial Enlargement (RAE) & Right Ventricular Hypertrophy (RVH) | RAE is recognized by the tall (>2.5mm) P waves in leads II, III, aVF. RVH is likely because of right axis deviation (+100 degrees) and the Qr (or rSR') complexes in V1-2. | Knowledge Weavers ECG | |
| 1203 |
 |
Frontal plane: accelerated junctional rhythm and inferior MI | Frontal plane: accelerated junctional rhythm and inferior MI | Knowledge Weavers ECG | |
| 1204 |
 |
QRS axis = -30 degrees | Lead II is isoelectric; I is positive; III is negative. The axis is -30 degrees. | Knowledge Weavers ECG | |
| 1205 |
 |
Voltage criteria for LVH | Voltage criteria for LVH | Knowledge Weavers ECG | |
| 1206 |
 |
Infero-posterior MI | Infero-posterior MI | Knowledge Weavers ECG | |
| 1207 |
 |
RBBB - marquette | RBBB - marquette | Knowledge Weavers ECG | |
| 1208 |
 |
Second degree AV block, type I, with bradycardia-dependent RBBB | An interesting and unusual form of rate-dependent bundle branch block. Normal sinus rhythm at 85 bpm is present with a 3:2 and 2:1 2nd degree AV block. The progressive PR prolongation in the 3:2 block makes this a type-I or Wenckebach block.Long cycles end in RBBB; short cycles have normal QRS dur... | Knowledge Weavers ECG | |
| 1209 |
 |
Bifascicular block: RBBB + LAFB | This is the most common of the bifascicular blocks. RBBB is most easily recognized in the precordial leads by the rSR' in V1 and the wide S wave in V6 (i.e., terminal QRS forces oriented rightwards and anterior). LAFB is best seen in the frontal plane leads as evidenced by left axis deviation (-50... | Knowledge Weavers ECG | |
| 1210 |
 |
Frontal plane lead diagram | The six frontal plane leads are illustrated with their respective positive and negative poles.When forced to intersect at a center point, the six leads inscribe a 360 degree circle. The normal frontal plane axis is from -30 degrees to + 90 degrees, shaded in grey. Left axis deviation is from -30 d... | Knowledge Weavers ECG | |
| 1211 |
 |
Anteroseptal MI: fully evolved | The QS complexes, resolving ST segment elevation and T wave inversions in V1-2 are evidence for a fully evolved anteroseptal MI. The inverted T waves in V3-5, I, aVL are also probably related to the MI. | Knowledge Weavers ECG | |
| 1212 |
 |
Atrial parasystole | The evenly spaced dots indicate ectopic atrial activity from a parasystolic atrial pacemaker. Non-fixed coupled PACs are seen having a common inter-ectopic interval. One of the PACs is nonconducted. | Knowledge Weavers ECG | |
| 1213 |
 |
Ventricular tachycardia - marquette | Ventricular tachycardia - marquette | Knowledge Weavers ECG | |
| 1214 |
 |
Long QT Iinterval | Long QT Interval | Knowledge Weavers ECG | |
| 1215 |
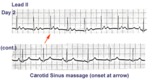 |
ECG of the century - part II: dual AV pathways | An astute cardiology fellow, yours truly, went to the patient's bedside on Day 2 and massaged the right carotid sinus as indicated by the arrow. Four beats later at a slightly slower heart rate the PR interval suddenly normalized suggesting an abrupt change from a slow AV nodal pathway to a fast AV... | Knowledge Weavers ECG | |
| 1216 |
 |
Left Atrial Enlargement & Nonspecific ST-T Wave Abnormalities | LAE is best seen in V1 with a prominent negative (posterior) component measuring 1mm wide and 1mm deep. There are also diffuse nonspecific ST-T wave abnormalities which must be correlated with the patient's clinical status. Poor R wave progression in leads V1-V3, another nonspecific finding, is als... | Knowledge Weavers ECG | |
| 1217 |
 |
Atrial flutter with 3:2 AV conduction | This 12-lead ECG shows a subtle bigeminal rhythm resulting from atrial flutter with a 3:2 AV conduction ratio; RR intervals alternate by a small duration. This is uncommon! The impulses from the atrial flutter conduct through the AV junction in a Wenckebach sequence; for every 3 flutter waves the s... | Knowledge Weavers ECG | |
| 1218 |
 |
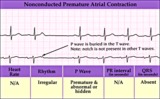
A very subtle 1st degree AV block | Where are the P waves??? They are hiding in the T waves as indicated by the arrows. How do we know? The PVC unmasked the sinus P wave, and now it is seen in the pause following the PVC. The PR interval is, therefore, about 500 ms. | Knowledge Weavers ECG | |
| 1219 |
 |
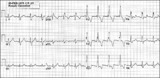
PAC's with and without aberrant conduction - marquette | PAC's with and without aberrant conduction - marquette | Knowledge Weavers ECG | |
| 1220 |
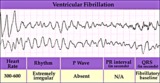 |
Ventricular fibrillation - marquette | Ventricular fibrillation - marquette | Knowledge Weavers ECG | |
| 1221 |
 |
Nonconducted PAC - marquette | Nonconducted PAC - marquette | Knowledge Weavers ECG | |
| 1222 |
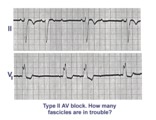 |
Trifascicular block: RBBB, LAFB, and mobitz II 2nd degree AV block | A nice example of trifascicular block: Lead V1 shows RBBB; Lead II is mostly negative with an rS morphology suggesting left anterior fascicular block. Since Mobitz II 2nd degree AV block is more often located in the bundle branch system, the only location left for this block is the left posterior ... | Knowledge Weavers ECG | |
| 1223 |
 |
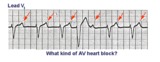
2nd degree AV block, type I, with junctional escapes | Junctional escapes are passive, protective events whenever the heart rate slows below that of the escape mechanism. In this example of 2nd degree AV block, type I, the escapes occur following the non-conducted P waves. Arrows indicate the position of the P waves. Note that the escape beats have a... | Knowledge Weavers ECG | |
| 1224 |
 |
Atrial flutter with 2:1 AV conduction | Atrial flutter with 2:1 AV block is one of the most frequently missed ECG rhythm diagnoses because the flutter waves are often hard to find. In this example two flutter waves for each QRS are best seen in lead III and V1. The ventricular rate at 150 bpm should always prompt us to consider atrial fl... | Knowledge Weavers ECG | |
| 1225 |
 |
Identification of PVC's and PAC's | PVC's usually stick out like sore thumbs; PAC's are often difficult to see because they are hidden in the preceding ST-T wave. The PVC in this example is mostly negative in lead V1 suggesting RV origin; i.e., most of activation is moving in posterior direction towards the left ventricle. | Knowledge Weavers ECG | |
| 1226 |
 |
AV dissociation by default | The nonconducted PAC's set up a long pause which is terminated by ventricular escapes; note the wider QRS morphology of the escape beats indicating their ventricular origin. Incomplete AV dissociation occurs during the escape beats, since the atria are still under the control of the sinus node. | Knowledge Weavers ECG | |
| 1227 |
 |
Lead error: V1 and V3 are transposed! | In the precordial leads the V1 and V3 chest electrodes are interchanged. Experienced ECG interpreters should be able to spot this lead placement error. | Knowledge Weavers ECG | |
| 1228 |
 |
Infero-posterior MI & RBBB: Frontal Plane Leads + V1 | Infero-posterior MI & RBBB: Frontal Plane Leads + V1 | Knowledge Weavers ECG | |
| 1229 |
 |
WPW Type Pre-excitation: Precordial Leads | WPW Type Pre-excitation: Precordial Leads | Knowledge Weavers ECG | |
| 1230 |
 |
Acute anterior MI | Acute anterior MI | Knowledge Weavers ECG | |
| 1231 |
 |
2nd degree AV block, type I with escapes and captures | Often in the setting of 2nd degree AV block the pauses caused by nonconducted P waves are long enough to enable escape pacemakers from the junction or ventricles to take over. This example illustrates junctional escapes, labled E and captures, labled C. Note that the PR intervals for the captures ... | Knowledge Weavers ECG | |
| 1232 |
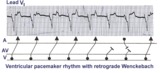 |
Ventricular paced rhythm with retrograde wenckebach | Retrograde atrial captures from a ventricular paced rhythm are occurring with increasing R-P intervals; i.e., retrograde Wenckebach. The ladder diagram indicates that after the blocked retrograde event, a single sinus P wave is seen dissociated from the ventricular rhythm. | Wenckebach AV Block | Knowledge Weavers ECG |
| 1233 |
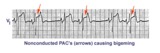 |
Nonconducted PAC's: an unusual bigeminy | Occasionally nonconducted PAC's can create interesting rhythms. In this example every other sinus beat is followed by an early, nonconducted PAC. The resulting pause sets up a bigeminal rhythm. Note the distortion of the T waves caused by the nonconducted PAC's. | Knowledge Weavers ECG | |
| 1234 |
 |
Atrial flutter with 2:1 AV conduction: leads II, III, V1 | In leads II and III, the one of the flutter waves occurs at the end of the QRS complex and might be mistaken for part of the QRS itself; i.e., the S wave. In lead V1, the two flutter waves for every QRS are more easily identified. | Knowledge Weavers ECG | |
| 1235 |
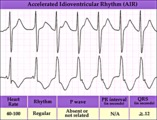 |
Accelerated IVR with AV dissociation - marquette | Accelerated IVR with AV dissociation - marquette | Knowledge Weavers ECG | |
| 1236 |
 |
Old inferior MI | Old inferior MI | Knowledge Weavers ECG | |
| 1237 |
 |
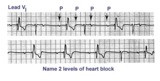
Diagram: type I vs. type II 2nd degree AV block | In type I 2nd degree AV block the PR progressively lengthens until a nonconducted P wave occurs. The PR gets longer by smaller and smaller increments; this results in gradual shortening of the RR intervals. The RR interval of the pause is usually less than the two preceding RR intervals. The RR i... | Knowledge Weavers ECG | |
| 1238 |
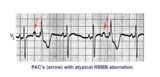 |
PAC's with RBBB aberration | These PAC's, indicated by arrows, enter the ventricles and find the right bundle refractory. They therefore conduct with RBBB aberrancy. In most normal hearts the right bundle recovery time is longer than the left bundle's; most aberrancy, therefore, has aRBBB morphology. In some diseased hearts t... | Knowledge Weavers ECG | |
| 1239 |
 |
RBBB + LAFB = bifascicular block | The RBBB is diagnosed by the wide QRS with prominent anterior (e.g., V1) and late rightward (e.g., I, V6) forces. The LAFB is recognized by the marked left axis deviation (-75 degrees) in the frontal plane, rS complexes in II, III, aVF, and the tiny q-wave in aVL. | Knowledge Weavers ECG | |
| 1240 |
 |
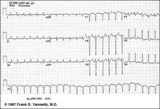
Massage parlor games | When unsure of the mechanism of a supraventricular tachycardia, carotid sinus massage may help make the diagnosis. In this example, carotid sinus massage causes marked AV block which permits easy recognition of the rapid, regular atrial flutter waves. | Knowledge Weavers ECG | |
| 1241 |
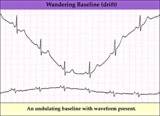 |
Wandering baseline artifact - marquette | Wandering baseline artifact - marquette | Knowledge Weavers ECG | |
| 1242 |
 |
Frontal plane QRS axis = +15 degrees | Frontal plane QRS axis = +15 degrees | Knowledge Weavers ECG | |
| 1243 |
 |
Frontal plane QRS axis = +30 degrees | Frontal plane QRS axis = +30 degrees | Knowledge Weavers ECG | |
| 1244 |
 |
Acute inferoposterior MI | Acute inferoposterior MI | Knowledge Weavers ECG | |
| 1245 |
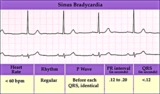 |
Sinus bradycardia | Sinus bradycardia | Knowledge Weavers ECG | |
| 1246 |
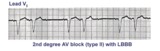 |
2nd degree AV block, mobitz type II, with LBBB | The wide QRS complexes in lead V1 indicates LBBB. 2nd degree AV block, Mobitz II is suggested by the two fixed PR intervals prior to the nonconducted P wave. The location of the block is most likely in the right bundle, because Mobitz II is usually a sign of bilateral bundle branch disease. | Knowledge Weavers ECG | |
| 1247 |
 |
A very subtle atrial tachycardia with 2:1 block | Although at first glance this looks like normal sinus rhythm at 95 bpm. On closer look, there are 2 P waves for every QRS; the atrial rate is 190 bpm. Note the hidden P in the T waves. This rhythm is likely due to digitalis intoxication, as are the GI symptoms. | Knowledge Weavers ECG | |
| 1248 |
 |
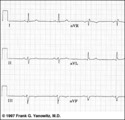
Left atrial enlargement | Left atrial enlargement is illustrated by increased P wave duration in lead II, top ECG, and by the prominent negative P terminal force in lead V1, bottom tracing. | Knowledge Weavers ECG | |
| 1249 |
 |
Acute postero-lateral MI: precordial leads | Acute postero-lateral MI: precordial leads | Knowledge Weavers ECG | |
| 1250 |
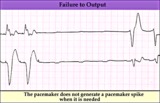 |
Pacemaker failure to pace - marquette | Pacemaker failure to pace - marquette | Knowledge Weavers ECG | |
| 1251 |
 |
Frontal plane QRS axis = 90 degrees | Frontal plane QRS axis = 90 degrees | Knowledge Weavers ECG | |
| 1252 |
 |
Junctional tachycardia - marquette | Junctional tachycardia - marquette | Knowledge Weavers ECG | |
| 1253 |
 |
Diagram: frontal plane leads | Diagram: frontal plane leads | Knowledge Weavers ECG | |
| 1254 |
 |
Inferoposterior MI | Inferoposterior MI | Knowledge Weavers ECG | |
| 1255 |
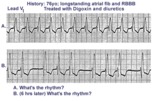 |
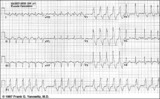
Digitalis intoxication: Junctional tachycardia with and without AV block | In a patient with longstanding atrial fibrillation being treated with digoxin, a regular tachycardia, as seen in A, with a RBBB suggests a junctional or supraventricular tachycardia. Group beating, in B, is likely due to a 2nd degree, Type 1, exit block below the ectopic junctional focus. This is h... | Knowledge Weavers ECG | |
| 1256 |
 |
Nonconducted PACs and junctional escapes | Although at first glance this looks like 2nd degree AV block, the P waves indicated by the arrows are premature and not sinus P waves. The pause is long enough to encourage a junctional escape focus to take over. Note the sinus P waves just before the escape beats. Had the escapes not occurred, t... | Knowledge Weavers ECG | |
| 1257 |
 |
WPW diagram | The short PR interval is due to a bypass track, also known as the Kent pathway. By bypassing the AV node the PR shortens. The delta wave represents early activation of the ventricles from the bypass tract. The fusion QRS is the result of two activation sequences, one from the bypass tract and one... | Knowledge Weavers ECG | |
| 1258 |
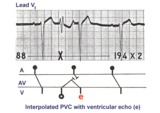 |
PVC with venticular echo | The PVC in this example retrogradely enters the AV junction and returns, usually down a different pathway, to reactivate the ventricles....a ventricular echo. This is unlikely to be an interpolated PVC because the PR interval following the PVC is too short for the sinus impulse to have entered the ... | Knowledge Weavers ECG | |
| 1259 |
 |
Left bundle branch block (LBBB) | LBBB is recognized by 1) QRS duration>0.12s; 2) monophasic R waves in I and V6; and 3) terminal QRS forces oriented leftwards and posterior. The ST-T waves should be oriented opposite to the terminal QRS forces. | Knowledge Weavers ECG | |
| 1260 |
|
PAC with RBBB aberrant conduction | PAC with RBBB aberrant conduction | Knowledge Weavers ECG | |
| 1261 |
 |
Interpolated PVCs - marquette | Interpolated PVCs - marquette | Knowledge Weavers ECG | |
| 1262 |
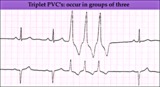 |
PVC triplet - marquette | PVC triplet - marquette | Knowledge Weavers ECG | |
| 1263 |
 |
Ventricular tachycardia with retrograde wenckebach | Approximately 50 percent of ventricular tachycardias are associated with AV dissociation. The other 50 percent have retrograde atrial capture. This example shows ventricular tachycardia with retrograde Wenckebach. The retrograde P waves are hard to find, but the arrows are of some help. | Wenckebach AV Block | Knowledge Weavers ECG |
| 1264 |
 |
Nonconducted and aberrantly conducted PAC's | In A the slow sinus rhythm is actually caused by nonconducted PACs hidden in the ST segment. This is confirmed in B where some of the PACs are aberrantly conducted with LBBB, and some PACs are nonconducted. | Knowledge Weavers ECG | |
| 1265 |
 |
Left anterior fasicular block: frontal plane leads | Left anterior fascicular block, LAFB, is recognized by left axis deviation of -45 degrees or greater; rS complexes in II, III, aVF; and a small Q wave in I and/or aVL. | Knowledge Weavers ECG | |
| 1266 |
 |
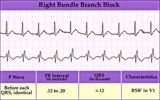
Right bundle branch block (RBBB) | Right bundle branch block (RBBB) | Knowledge Weavers ECG | |
| 1267 |
 |
All about premature beats | All about premature beats | Knowledge Weavers ECG | |
| 1268 |
 |
Inferoposterior MI | Inferoposterior MI | Knowledge Weavers ECG | |
| 1269 |
 |
Sino-atrial exit block, type I or wenckebach | This example illustrates 2nd degree sino-atrial exit block. In type 1 S-A block the conduction time between sinus firing and atrial capture progressively prolong, but this cannot be seen on the ECG tracing; type I exit block is inferred if the P-P intervals gradually shorten before the pause and if... | Wenckebach AV Block; Ladder Diagram | Knowledge Weavers ECG |
| 1270 |
 |
Inferior & Anteroseptal MI + RBBB | Pathologic Q waves are seen in leads II, III, aVF (inferior MI) and in leads V1-3 (anteroseptal MI). RBBB is recognized by the wide QRS (>0.12s) and the anterior/rightwards orientation of terminal QRS forces. When an anteroseptal MI complicates RBBB (or visa versa) the rSR' complex in V1 (typical ... | Knowledge Weavers ECG | |
| 1271 |
 |
Atrial flutter with 3:2 conduction ratio: frontal plane leads | Note the subtle bigeminy in the RR intervals. The best way to identify the flutter waves in this example is to imagine what lead III would look like if the QRS complexs disappeared; what remains is a reasonable saw-tooth pattern characteristic of atrial flutter with a flutter rate of about 300 bpm... | Knowledge Weavers ECG | |
| 1272 |
 |
Accelerated ventricular rhythm with retrograde atrial capture and echo beats | Retrograde atrial captures from an accelerated ventricular focus are occurring with increasing R-P intervals, When the longer R-P occurs, the impulse traversing the AV junction finds a route back to the ventricles, and the result is a ventricular echo. | Knowledge Weavers ECG | |
| 1273 |
 |
ECG components diagram - marquette | ECG components diagram - marquette | Knowledge Weavers ECG | |
| 1274 |
 |
Postero-lateral MI: Precordial Leads | Postero-lateral MI: Precordial Leads | Knowledge Weavers ECG | |
| 1275 |
 |
Indeterminate frontal plane QRS axis | Indeterminate frontal plane QRS axis | Knowledge Weavers ECG | |
| 1276 |
 |
PAC couplet - marquette | PAC couplet - marquette | Knowledge Weavers ECG | |
| 1277 |
 |
Normal variant: Early repolarization | Early repolarization, a misnomer, describes a pattern of localized or diffuse ST segment elevation. This is especially seen in leads with prominent R waves. In this example leads I, II, V5 and V6 illustrate the early repolarization pattern. ST segments usually have a concave upwards pattern and ta... | Knowledge Weavers ECG | |
| 1278 |
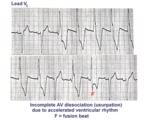 |
AV dissociation by usurpation | Normal sinus rhythm is interrupted by an accelerated ventricular rhythm whose rate is slightly faster than the sinus rhythm. Fusion QRS complexes occur whenever the sinus impulse enters the ventricles at the same time the ectopic ventricular focus initiates its depolarization. | Knowledge Weavers ECG | |
| 1279 |
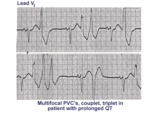 |
Long QT mischief | The long QT ECG has many causes: electrolyte abnormalities including hypo-K, hypo-Mg, and hypo-Ca; drugs including type I antiarrhythmics; CNS injury; and hereditary syndromes. Ventricular arrhythmias are thought to be caused by afterdepolarizations or triggered automaticity. | Knowledge Weavers ECG | |
| 1280 |
 |
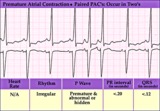
Nonconducted and conducted PAC's | The pause in this example is the result of a nonconducted PAC, as indicated by the first arrow. The second arrow points to a conducted PAC. The most common cause of an unexpected pause in rhythm is a nonconducted PAC. | Knowledge Weavers ECG | |
| 1281 |
 |
Atypical LBBB with Q waves in leads I and aVL | In typical LBBB, there are no initial Q waves in leads I, aVL, and V6. If Q waves are present in 2 or more of these leads, myocardial infarction is present. | Knowledge Weavers ECG | |
| 1282 |
 |
Old inferior MI, PVCs, and atrial fibrillation | Old inferior MI, PVCs, and atrial fibrillation | Knowledge Weavers ECG | |
| 1283 |
 |
Frontal plane QRS axis = -45 degrees | Frontal plane QRS axis = -45 degrees | Knowledge Weavers ECG | |
| 1284 |
 |
LVH & PVCs: Precordial Leads | LVH & PVCs: Precordial Leads | Knowledge Weavers ECG | |
| 1285 |
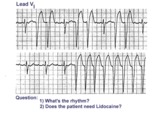 |
Atrial flutter with variable AV block and rate-dependent LBBB | The basic rhythm is atrial flutter with variable AV block. When 2:1 conduction ratios occur there is a rate-dependent LBBB. Don't be fooled by the wide QRS tachycardia on the bottom strip. It's not ventricular tachycardia, but atrial flutter with 2:1 conduction and LBBB. Lidocaine is not needed ... | Knowledge Weavers ECG | |
| 1286 |
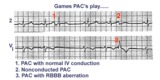 |
three fates of PAC's | As illustrated, PAC's can have three fates: PAC-1enters the ventricles and encounters no conduction delays, therefore causing a narrow QRS; PAC-2 occurs a little earlier and can't get through the AV junction, therefore beingnonconducted; PAC-3 seen inlead V1 makes it into the ventricles but encounte... | Knowledge Weavers ECG | |
| 1287 |
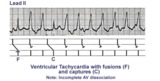 |
Ventricular tachycardia with AV dissociation, captures, and fusions | Approximately 50 percent of ventricular tachycardias are associated with AV dissociation. In these cases atrial impulses can enter the ventricles and either fuse with a ventricular ectopic beat or completely capture the ventricles. This ladder diagram illustrates these events. | Knowledge Weavers ECG | |
| 1288 |
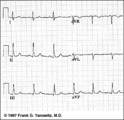 |
Frontal plane QRS axis = +75 degrees | Since there is no isoelectric lead in this ECG, the two closest leads are I and aVL. If I were isoelectric, the axis would be +90 degrees; if aVL were isoelectric, the axis would be +60 degrees. A nice compromize is +75 degrees. (The two closest leads are always 30 degrees apart.) | Knowledge Weavers ECG | |
| 1289 |
 |
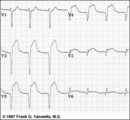
Right axis deviation: QRS axis = +130 degrees | Lead aVR is almost isoelectric; lead I is mostly negative, and lead III is very positive. The QRS axis, therefore, is +130 degrees. Note that the slightly more positive AVR moves the axis slightly beyond +120 degrees; i.e., closer to the + pole of the aVR lead. | Knowledge Weavers ECG | |
| 1290 |
 |
Extensive anterior/anterolateral MI: precordial leads | Extensive anterior/anterolateral MI: precordial leads | Knowledge Weavers ECG | |
| 1291 |
 |
LVH: strain pattern + left atrial enlargement | LVH: strain pattern + left atrial enlargement | Knowledge Weavers ECG | |
| 1292 |
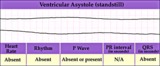 |
Ventricular asystole - marquette | Ventricular asystole - marquette | Knowledge Weavers ECG | |
| 1293 |
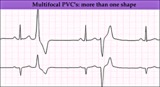 |
Multifocal PVC's - marquette | Multifocal PVC's - marquette | Knowledge Weavers ECG | |
| 1294 |
 |
Atrial flutter with 2:1 AV conduction | In this example of atrial flutter with 2:1 AV conduction the flutter waves are very hard to see. Atrial flutter with 2:1 block must be considered, however, because the heart rate is about 150 bpm. A careful look at V1 shows the two flutter waves for each QRS complex complex. One flutter wave imme... | Knowledge Weavers ECG | |
| 1295 |
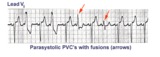 |
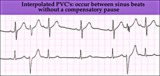
Ventricular parasystole | In ventricular parasystole, non-fixed coupled PVC's occur at a common inter-ectopic interval. Fusion beats, indicated by arrows, are often seen. Fusions occur when the sinus impulse entering the ventricles find the ventricles already partially depolarized by the parasystolic focus. | Knowledge Weavers ECG | |
| 1296 |
 |
Atrial flutter with 2:1 and 4:1 conduction and rate dependent LBBB | In this example of atrial flutter with variable AV conduction, the faster rates are associated with rate-related LBBB. Don't confuse this for ventricular tachycardia. | Knowledge Weavers ECG | |
| 1297 |
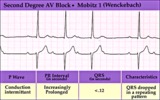 |
2nd degree AV block, type I (Wenckebach) | 2nd degree AV block, type I (Wenckebach) | Knowledge Weavers ECG | |
| 1298 |
 |
Diagram: stages of acute Q-wave MI | Diagram: stages of acute Q-wave MI | Knowledge Weavers ECG | |
| 1299 |
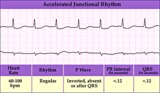 |
Accelerated junctional rhythm | Accelerated junctional rhythm | Knowledge Weavers ECG | |
| 1300 |
 |
PVC's - marquette | PVC's - marquette | Knowledge Weavers ECG |