The Health Education Assets Library (HEAL) is a collection of over 22,000 freely available digital materials for health sciences education. The collection is now housed at the University of Utah J. Willard Marriott Digital Library.
TO
Filters: Collection: "ehsl_heal"
| Title | Description | Subject | Collection | ||
|---|---|---|---|---|---|
| 1101 |
 |
LVH and many PVCs | The combination of voltage criteria (SV2 + RV6>35mm) and ST-T abnormalities in V5-6 are definitive for LVH. There may also be LAE as evidenced by the prominent negative P terminal force in lead V1. Isolated PVCs and a PVC couplet are also present. | Knowledge Weavers ECG | |
| 1102 |
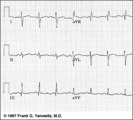 |
Frontal plane QRS axis = +150 degrees (RAD) | This is an unusual right axis deviation (RAD). Lead I is negative, which usually means RAD. Lead II is the isoelectric lead, which almost always means -30 degrees; but in this example the axis is 180 degrees away from -30, or +150 degrees. | Knowledge Weavers ECG | |
| 1103 |
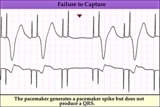 |
Pacemaker failure to capture - marquette | Pacemaker failure to capture - marquette | Knowledge Weavers ECG | |
| 1104 |
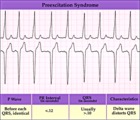 |
WPW type preexcitation - marquette | WPW type preexcitation - marquette | Knowledge Weavers ECG | |
| 1105 |
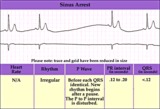 |
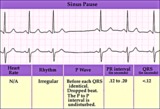
Sinus pause or arrest - marquette | Sinus pause or arrest - marquette | Knowledge Weavers ECG | |
| 1106 |
 |
SA exit block - marquette | SA exit block - marquette | Knowledge Weavers ECG | |
| 1107 |
 |
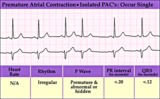
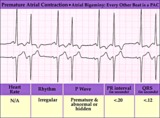
An interpolated PAC | Although most PACs reset the sinus node producing an incomplete compensatory pause, this PAC, indicated by the black arrow, is interpolated, i.e., sandwiched between two sinus beats. Note that the subsequent sinus P wave conducts with prolonged PR interval due to the relative refractoriness of the... | Knowledge Weavers ECG | |
| 1108 |
 |
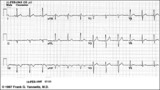
Incomplete AV dissociation due To 2nd degree AV block | 2nd degree AV block is evident from the nonconducted P waves. Junctional escapes, labled J, terminate the long pauses because that's the purpose of escape pacemakers....to protect us from too slow heart rates. All QRSs with shorter RR intervals are capture beats, labeled c. Atypical RBBB with a q... | Knowledge Weavers ECG | |
| 1109 |
 |
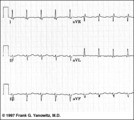
Frontal plane QRS axis = +50 degrees | 1) lead aVL is the smallest QRS and closest to being the isoelectric lead; 2) perpendiculars to aVL are +60 and -120 degrees; 3) lead I is positive; 4) therefore, the axis is closest to being +60 degrees. Because aVL is actually slightly positive, the axis is only about +50 degrees (i.e., slightly ... | Knowledge Weavers ECG | |
| 1110 |
 |
Atypical LBBB with primary T wave abnormalities | Primary T wave abnormalities in LBBB refer to T waves in the same direction as the major deflection of the QRS. These are seen in leads I, III, aVL, V2-4. Most likely diagnosis is myocardial infarction. | Knowledge Weavers ECG | |
| 1111 |
 |
Mobitz II 2nd degree AV block with LBBB | The QRS morphology in lead V1 shows LBBB. The arrows point to two consecutive nonconducted P waves, most likely hung up in the diseased right bundle branch. This is classic Mobitz II 2nd degree AV block. | Knowledge Weavers ECG | |
| 1112 |
 |
RBBB with primary ST-T abnormalities: Precordial leads | RBBB with primary ST-T abnormalities: Precordial leads | Knowledge Weavers ECG | |
| 1113 |
 |
Bifascicular block: RBBB + LAFB | Bifascicular block: RBBB + LAFB | Knowledge Weavers ECG | |
| 1114 |
 |
PVC with R-on-T - marquette | PVC with R-on-T - marquette | Knowledge Weavers ECG | |
| 1115 |
 |
PVCs - marquette | PVCs - marquette | Knowledge Weavers ECG | |
| 1116 |
 |
Right Ventricular Hypertrophy (RVH) & Right Atrial Enlargement (RAE) | In this case of severe pulmonary hypertension, RVH is recognized by the prominent anterior forces (tall R waves in V1-2), right axis deviation (+110 degrees), and P pulmonale (i.e., right atrial enlargement). RAE is best seen in the frontal plane leads; the P waves in lead II are >2.5mm in amplitud... | Knowledge Weavers ECG | |
| 1117 |
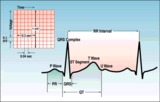 |
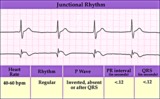
ECG intervals and waves | The P wave represents atrial activation; the PR interval is the time from onset of atrial activation to onset of ventricular activation. The QRS complex represents ventricular activation; the QRS duration is the duration of ventricular activation. The ST-T wave represents ventricular repolarizatio... | Knowledge Weavers ECG | |
| 1118 |
 |
Atrial flutter with 2:1 AV conduction | Flutter waves are best seen in lead V1; one immediately follows the QRS and the other precedes the next QRS. The regular ventricular rate of 150 bpm should always prompt us to condider this diagnosis. | Knowledge Weavers ECG | |
| 1119 |
 |
Left axis deviation: QRS axis = -45 degrees | There is no isoelectric, but leads aVR and II are the closest to being isoelectric, placing the axis between -30 and -60 degrees. The axis, therefore, is about -45 degrees. | Knowledge Weavers ECG | |
| 1120 |
 |
Long QT: an ECG marker for sudden cardiac death | Long QT: an ECG marker for sudden cardiac death | Knowledge Weavers ECG | |
| 1121 |
 |
Frontal plane QRS axis = 0 degrees | Frontal plane QRS axis = 0 degrees | Knowledge Weavers ECG | |
| 1122 |
 |
Isolated PAC - marquette | Isolated PAC - marquette | Knowledge Weavers ECG | |
| 1123 |
 |
Inferolateral ST segment elevation | ST Segment elevation with a straight or convex upwards configuration usually means transmural ischemia (or injury) and is seen in the setting of acute myocardial infarction. This ECG finding may also be seen transiently during coronary artery spasm. Unlike ST depression, ST elevation is often loca... | Knowledge Weavers ECG | |
| 1124 |
 |
A PAC initiates paroxysmal atrial fibrillation | The arrow indicates slight alteration of the ST-T wave by a PAC. The PAC, in turn, falls during the vulnerable period of atrial repolarization and initiates atrial fibrillation. Similar but more catastrophic events happen in the ventricles when PVC's occur during the vulnerable period, i.e. R-on-T... | Knowledge Weavers ECG | |
| 1125 |
 |
Left Atrial Abnormality & 1st Degree AV Block | The P-wave is notched, wider than 0.12s, and has a prominent negative (posterior) component in V1 - all criteria for left atrial abnormality or enlargement (LAE). The PR interval >0.20s. Minor ST-T wave abnormalities are also present. | Knowledge Weavers ECG | |
| 1126 |
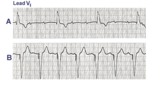 |
3rd degree AV block rx'ed with a ventricular pacemaker | In A the ECG shows complete or 3rd degree AV block with a left ventricular escape rhythm, as evidenced by the upright QRS morphology. In B the artificial right ventricular pacemaker rhythm is shown. | Knowledge Weavers ECG | |
| 1127 |
 |
Lead Error: V1 & V3 are Transposed | In this normal 12-lead ECG the V1 and V3 chest electrodes are interchanged. Experienced ECG interpreters should be able to spot this lead placement error. | Knowledge Weavers ECG | |
| 1128 |
 |
PAC and PVC: complete vs. incomplete pause | PAC and PVC: complete vs. incomplete pause | Knowledge Weavers ECG | |
| 1129 |
 |
Electronic atrial pacing - marquette | Electronic atrial pacing - marquette | Knowledge Weavers ECG | |
| 1130 |
 |
Normal sinus rhythm - marquette | Normal sinus rhythm - marquette | Knowledge Weavers ECG | |
| 1131 |
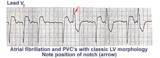 |
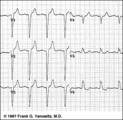
Left ventricular PVC's | In lead V1, these PVC's are positive or anterior in direction indicating probable LV origin with late activation of the right ventricle. The arrow points to the notch on the downstroke of the PVC making its morphology highly unlikely to be an aberrantly conducted supraventricular beat. | Knowledge Weavers ECG | |
| 1132 |
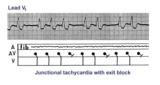 |
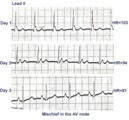
Junctional tachycardia with exit block: a manifestation of digitalis intoxication | Theladder diagramsays it all: the atria are fibrillating; there is complete heart block in the AV junction; a junctional tachycardia focus is firing at about 130 bpm, but not all junctional impulses reach the ventricles due to 2nd degree exit block. | Knowledge Weavers ECG | |
| 1133 |
 |
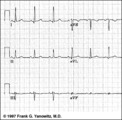
Frontal plane QRS axis = +90 degrees | 1) Lead I is isoelectric; 2) perpendiculars to lead I are +90 and -90 degrees; 3) leads II, III, aVF are positive; 4) therefore, the axis must be +90 degrees. | Knowledge Weavers ECG | |
| 1134 |
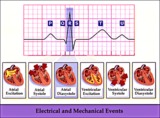 |
Electrical and mechanical events diagram - marquette | Electrical and mechanical events diagram - marquette | Knowledge Weavers ECG | |
| 1135 |
 |
Anteroseptal MI, fully evolved: precordial leads | Anteroseptal MI, fully evolved: precordial leads | Knowledge Weavers ECG | |
| 1136 |
 |
Left atrial enlargement: leads II and V1 | Left atrial enlargement: leads II and V1 | Knowledge Weavers ECG | |
| 1137 |
 |
Fully evolved inferior MI: frontal plane | Fully evolved inferior MI: frontal plane | Knowledge Weavers ECG | |
| 1138 |
 |
Frontal plane QRS axis = -75 degrees | Frontal plane QRS axis = -75 degrees | Knowledge Weavers ECG | |
| 1139 |
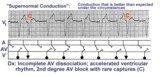 |
Supernormal conduction: 2nd degree AV block with rare captures; accelerated ventricular rhythm | This complicated rhythm strip illustrates 'supernormal' conduction... a situation where conduction is better than expected. The ladder diagram shows that the accelerated ventricular rhythm prevents most of the sinus impulses from reaching the ventricles. Only appropriately timed sinus impulses rea... | Knowledge Weavers ECG | |
| 1140 |
 |
Complete AV block, junctional escape rhythm, and ventriculophasic sinus arrhythmia | Complete AV block is seen as evidenced by the AV dissociation. A junctional escape rhythm sets the ventricular rate at 45 bpm. The PP intervals vary because of ventriculophasic sinus arrhythmia; this is defined when the PP interval that includes a QRS is shorter than a PP interval that excludes a ... | Knowledge Weavers ECG | |
| 1141 |
 |
Junctional parasystole and pseudo-AV block | This complicated rhythm strip shows normal sinus rhythm and a competing junctional parasystolic focus. Solid circles indicate junctional premature beats from the parasystolic focus. Open circles indicate non-conducted junctional prematures; the first open circle is a nonconducted junctional prematur... | Knowledge Weavers ECG | |
| 1142 |
 |
Premature junctional complexes with retrograde P waves | The ladder diagram illustrates the PJC with retrograde atrial capture | Knowledge Weavers ECG | |
| 1143 |
 |
Left Atrial Abnormality & 1st Degree AV Block: Leads II and V1 | Left Atrial Abnormality & 1st Degree AV Block: Leads II and V1 | Knowledge Weavers ECG | |
| 1144 |
 |
Right Axis Deviation & RAE (P pulmonale): Leads I, II, III | Right Axis Deviation & RAE (P pulmonale): Leads I, II, III | Knowledge Weavers ECG | |
| 1145 |
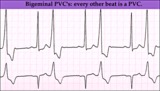 |
Ventricular bigeminy - marquette | Ventricular bigeminy - marquette | Knowledge Weavers ECG | |
| 1146 |
 |
LBBB and 2nd degree AV block, mobitz type I | Mobitz II 2nd degree AV block is usually a sign of bilateral bundle branch disease. One of the two bundle branches should be completely blocked; in this example the left bundle is blocked. The nonconducted sinus P waves are most likely blocked in the right bundle which exhibits 2nd degree block. ... | Knowledge Weavers ECG | |
| 1147 |
 |
Infero-posterior MI&RBBB | Deep Q waves in II, III, aVF plus tall R waves in V1-2 are evidence for this infero-posterior MI. The wide QRS (>0.12s) and RR' complex in V1 are evidence for RBBB. Any time RBBB has an initial R in V1 equal to or greater than the R', true posterior MI must be considered. Q waves in V5-6 suggest a... | Knowledge Weavers ECG | |
| 1148 |
 |
Extensive anterior/anterolateral MI: recent | Significant pathologic Q-waves (V2-6, I, aVL) plus marked ST segment elevation are evidence for this large anterior/anterolateral MI. The exact age of the infarction cannot be determined without clinical correlation and previous ECGs, but this is likely a recent MI. | Knowledge Weavers ECG | |
| 1149 |
 |
Nonconducted PAC's slowing the heart rate | Consecutive nonconducted PAC's, indicated by arrows, can significantly slow the heart rate. Note the distortion of the ST-T waves caused by the PAC. A hint in recognizing nonconducted PAC's is to find conducted PAC's in the same rhythm strip. | Knowledge Weavers ECG | |
| 1150 |
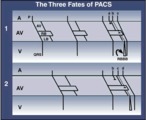 |
three fates of PAC's: 1. normal conduction; 2. aberrant conduction; 3. non-conduction | three fates of PAC's: 1. normal conduction; 2. aberrant conduction; 3. non-conduction | Knowledge Weavers ECG | |
| 1151 |
 |
QRS axis = 0 degrees | Lead aVF is isoelectric; lead I is positive; therefore, the QRS axis is 0 degrees. | Knowledge Weavers ECG | |
| 1152 |
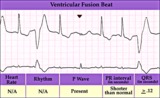 |
Ventricular fusion beat - marquette | Ventricular fusion beat - marquette | Knowledge Weavers ECG | |
| 1153 |
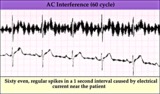 |
60 cycle artifact - marquette | 60 cycle artifact - marquette | Knowledge Weavers ECG | |
| 1154 |
 |
LBBB: precordial leads | LBBB: precordial leads | Knowledge Weavers ECG | |
| 1155 |
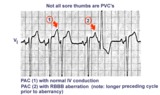 |
Not all sore thumbs are ventricular in origin | PACs have three fates: normal conduction into ventricles, aberrant conduction in ventricles due to bundle branch or fascicular block, and non-conduction due to block in AV junction. In this example PAC 1 is normally conducted and PAC 2 is conducted with RBBB aberration. The longer preceding cycle ... | Knowledge Weavers ECG | |
| 1156 |
 |
Acute infero-postero-lateral MI | Hyperacute ST segment elevation is seen in leads II, III, aVF (inferior location) and in leads V4-6 (apical lateral wall location). Hyperacute ST depression is seen in leads V1-2 (an expression of posterior wall injury). in addition there are reciprocal ST segment depression changes in leads I an... | Knowledge Weavers ECG | |
| 1157 |
 |
Ventricular Pacemaker Rhythm: V1-3 | Note the small pacemaker spikes before the QRS complexes. In addition, the QRS complex in V1-3 exhibits ventricular ectopic morphology; i.e., there is a slur or notch at the beginning of the S wave, and >60ms delay from onset to QRS to nadir of S wave. This rules against a supraventricular rhythm wi... | Knowledge Weavers ECG | |
| 1158 |
 |
Inferior MI: fully evolved | Significant pathologic Q-waves are seen in leads II, III, aVF along with resolving ST segment elevation and symmetrical T wave inversion. This is a classic inferior MI. | Knowledge Weavers ECG | |
| 1159 |
 |
Complete AV block (3rd degree) with junctional rhythm | Complete AV block (3rd degree) with junctional rhythm | Knowledge Weavers ECG | |
| 1160 |
 |
QRS axis = +90 degrees | Lead I is isoelectric; II and III are positive; the axis is +90 degrees. | Knowledge Weavers ECG | |
| 1161 |
 |
Left bundle branch block - marquette | Left bundle branch block - marquette | Knowledge Weavers ECG | |
| 1162 |
 |
Junctional escape rhythm | Junctional escape rhythm | Knowledge Weavers ECG | |
| 1163 |
 |
Diagram: AV nodal reentrant tachycardia | The AV node often has dual pathways; in this diagram the alpha pathway is fast, but has a long refractory period; the beta pathway is conducts more slowly, but recovers faster.In sinus rhythm the faster alpha pathway is used and accounts for the normal PR interval. When a PAC occurs, however, the i... | Knowledge Weavers ECG | |
| 1164 |
 |
Atrial parasystole | In atrial parasystole non-fixed coupled PACs, shown by arrows, occur at a common inter-ectopic interval or at multiples of this interval. Atrial fusions, not shown here, may also occur when the PAC occurs in close temporal proximity to the sinus impulse. | Knowledge Weavers ECG | |
| 1165 |
 |
Atrial flutter with 2:1 conduction: leads II, III, V1 | Atrial flutter with 2:1 conduction: leads II, III, V1 | Knowledge Weavers ECG | |
| 1166 |
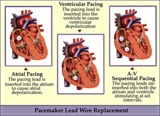 |
Pacemaker lead wire placement diagram - marquette | Pacemaker lead wire placement diagram - marquette | Knowledge Weavers ECG | |
| 1167 |
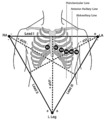 |
Frontal and horizontal plane lead diagram | Frontal and horizontal plane lead diagram | Knowledge Weavers ECG | |
| 1168 |
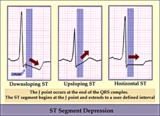 |
ST segment diagram - marquette | ST segment diagram - marquette | Knowledge Weavers ECG | |
| 1169 |
 |
Atrial bigeminy - marquette | Atrial bigeminy - marquette | Knowledge Weavers ECG | |
| 1170 |
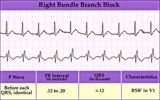 |
Right Bundle Branch Block | Right Bundle Branch Block | Knowledge Weavers ECG | |
| 1171 |
 |
2nd degree AV block, type I, with accelerated junctional escapes and a ladder diagram | The ladder diagram illustrates a Wenckebach type AV block by the increasing PR intervals before the blocked P wave. After the blocked P wave, however, a rev-ed up junctional pacemaker terminates the pause. Note that the junctional beats have a slightly different QRS morphology from the sinus beats... | Knowledge Weavers ECG | |
| 1172 |
 |
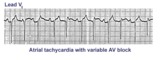
Atrial tachycardia with exit block and AV block | The ectopic P waves, easily seen in this example,occur in groups, separated by short pauses. This is likely due to an exit block just distal to the atrial pacemaker. Because not all of the P waves make it to the ventricles, there is also 2nd degree AV block. Therefore, two levels of block are pre... | Knowledge Weavers ECG | |
| 1173 |
 |
LVH | In this example of LVH, the precordial leads don't meet the usual voltage criteria or exhibit significant ST segment abnormalities. The frontal plane leads, however, show voltage criteria for LVH and significant ST segment depression in leads with tall R waves. The voltage criteria include 1) R in a... | Knowledge Weavers ECG | |
| 1174 |
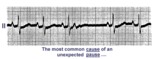 |
A nonconducted PAC causes an unexpected pause | Unexpected pauses in rhythm have several causes, the most frequent being a nonconducted PAC. In this example the nonconducted PAC is seen in the ST segment of the pause. Note the change in the ST-T compared to the other ST-T waves. | Knowledge Weavers ECG | |
| 1175 |
 |
Giant TU fusion waves | TU fusion waves are often seen in long QT syndromes. The differential diagnosis of this ECG abnormality includes electrolyte abnormalities -hypokalemia, CNS disease, e.g., subarachnoid hemorrhage; hereditary long QT syndromes, and drugs such as quinidine. | Knowledge Weavers ECG | |
| 1176 |
 |
Left anterior fascicular block (LAFB) | LAFB is the most common of the intraventricular conduction defects. It is recognized by 1) left axis deviation; 2) rS complexes in II, III, aVF; and 3) small q in I and/or aVL. | Knowledge Weavers ECG | |
| 1177 |
 |
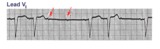
Atrial flutter with 2:1 AV conduction: lead V1 | The arrows point to two flutter waves for each QRS complex. Atrial rate = 280; ventricular rate = 140. | Knowledge Weavers ECG | |
| 1178 |
 |
Long QT Interval and Giant Negative T Waves | Long QT Interval and Giant Negative T Waves | Knowledge Weavers ECG | |
| 1179 |
 |
Frontal plane QRS axis = -15 degrees | Frontal plane QRS axis = -15 degrees | Knowledge Weavers ECG | |
| 1180 |
 |
Ventricular pacemaker rhythm | Note the small pacemaker spikes before the QRS complexes in many of the leads. In addition, the QRS complex in V1 exhibits ventricular ectopic morphology; i.e., there is a slur or notch at the beginning of the S wave, and>60ms delay from onset to QRS to nadir of S wave. This rules against a suprav... | Knowledge Weavers ECG | |
| 1181 |
 |
Diffuse anterolateral T wave abnormalities | Diffuse anterolateral T wave abnormalities | T Wave Abnormalities | Knowledge Weavers ECG |
| 1182 |
 |
Frontal plane QRS axis = -45 degrees | Frontal plane QRS axis = -45 degrees | Knowledge Weavers ECG | |
| 1183 |
 |
Marked sinus arrhythmia - marquette | Marked sinus arrhythmia - marquette | Knowledge Weavers ECG | |
| 1184 |
 |
Muscle tremor artifact - marquette | Muscle tremor artifact - marquette | Knowledge Weavers ECG | |
| 1185 |
 |
RBBB + LAFB: bifascicular block | RBBB + LAFB: bifascicular block | Knowledge Weavers ECG | |
| 1186 |
 |
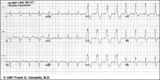
ECG of the century: A most unusual 1st degree AV block | On Day 1, at a heart rate of 103 bpm the P waves are not clearly defined suggesting an accelerated junctional rhythm. However, on Day 2, at a slightly slower heart rate the sinus P wave suddenly appears immediately after the QRS complex. In retrospect, the sinus P wave in Day 1 was found burried i... | Knowledge Weavers ECG | |
| 1187 |
 |
RBBB plus mobitz II 2nd degree AV block | The classic rSR' in V1 is RBBB. Mobitz II 2nd degree AV block is present because the PR intervals are constant. Statistically speaking, the location of the 2nd degree AV block is in the left bundle branch rather than in the AV junction. The last QRS in the top strip is a junctional escape, since... | Knowledge Weavers ECG | |
| 1188 |
 |
Left axis deviation: QRS axis = -60 degrees | Lead aVR is isoelectric; leads II and III are mostly negative. The QRS axis, therefore, is -60 degrees. | Knowledge Weavers ECG | |
| 1189 |
 |
QRS axis = +30 degrees | Lead III is isoelectric; leads I and II are positive. The QRS axis, therefore, is +30 degrees. | Knowledge Weavers ECG | |
| 1190 |
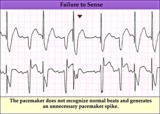 |
Pacemaker failure to sense - marquette | Pacemaker failure to sense - marquette | Knowledge Weavers ECG | |
| 1191 |
 |
Pacemaker fusion beat - marquette | Pacemaker fusion beat - marquette | Knowledge Weavers ECG | |
| 1192 |
 |
RAE & RVH | RAE & RVH | Knowledge Weavers ECG | |
| 1193 |
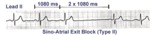 |
Type II, 2nd degree sino-atrial block | Two types of 2nd degree SA block have been described. In type-I, or SA Wenckebach, the P-P interval of the pause is less than 2x the preceding P-P intervals. In type-II SA block the P-P interval of the pause is approximately 2x the normal P-P interval. The distinction between types I and II is no... | Knowledge Weavers ECG | |
| 1194 |
 |
Bradycardia-dependent LBBB with carotid sinus massage | When carotid sinus massage slows the heart rate in this example, the QRS widens into a LBBB. This form of rate-dependent bundle branch block is thought to be due to latent pacemakers in the bundle undergoing phase 4 depolarization; when the sinus impulse enters the partially depolarized bundle, slow... | Knowledge Weavers ECG | |
| 1195 |
 |
Atrial tachycardia with 3:2 AV block | In this rhythm the atrial rate from an ectopic focus is 160 bpm. Atrial activity can be seen on top of T waves, and before QRS's. Careful observation reveals a 3:2 Wenckebach relationship between P waves and QRS's. Atrial tachycardia with block is often a sign of digitalis intoxication. | Knowledge Weavers ECG | |
| 1196 |
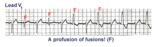 |
Ventricular fusion beats | Fusion beats occur when two or more activation fronts contribute to the electrical event. These may occur in the atria or in the ventricles. In this example the ventricular fusions are the result of simultaneous activation of the ventricles from two foci, the sinus node and a ventricular ectopic... | Knowledge Weavers ECG | |
| 1197 |
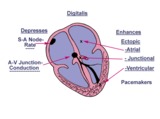 |
Diagram: digitalis effect on rhythm and conduction | Diagram: digitalis effect on rhythm and conduction | Knowledge Weavers ECG | |
| 1198 |
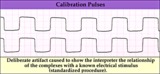 |
Calibration signal - marquette | Calibration signal - marquette | Knowledge Weavers ECG | |
| 1199 |
 |
Old inferior MI | Old inferior MI | Knowledge Weavers ECG | |
| 1200 |
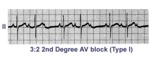 |
Second degree AV block, type I, with 3:2 conduction ratio | There are two types of 2nd degree AV Block. In this example of Type I or Wenckebach AV block there are 3 P waves for every 2 QRSs; the PR interval increases until a P wave fails to conduct. This is an example of group beating. | Knowledge Weavers ECG |