John A. Moran Eye Center Neuro-Ophthalmology Collection: A variety of lectures, videos and images relating to topics in Neuro-Ophthalmology created by faculty at the Moran Eye Center, University of Utah, in Salt Lake City.
NOVEL: https://novel.utah.edu/
TO
| Title | Description | Type | ||
|---|---|---|---|---|
| 1 |
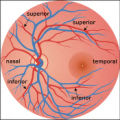 |
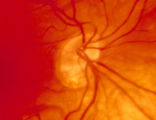
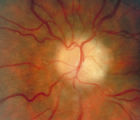
2-37a - Vascular Features | When looking at the disc, the central retinal artery and vein should be visible. The central retinal artery is usually slightly narrower than the vein. When the central retinal artery goes though the lamina cribrosa, the artery becomes smaller because of diminution of the muscular layer and loss of ... | Image |
| 2 |
 |
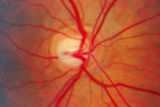
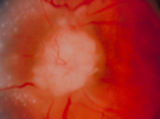
2-37b - Vascular Features | When looking at the disc, the central retinal artery and vein should be visible. The central retinal artery is usually slightly narrower than the vein. When the central retinal artery goes though the lamina cribrosa, the artery becomes smaller because of diminution of the muscular layer and loss of ... | Image |
| 3 |
 |
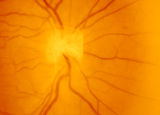
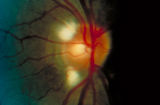
2-4a - Disc Anatomy | The optic disc appearance is determined by: the size of the eye, the size of the scleral canal, how the nerve is inserted into the globe, the appearance of the lamina cribrosa, where myelination stops, and what is left behind in normal development. Even though this is a disc with a very large cup, i... | Image |
| 4 |
 |
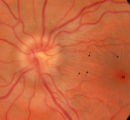
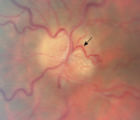
2-53a - Venous Pulsations | On the disc, look for spontaneous venous pulsations. Spontaneous venous pulsations can be seen in the large trunks of veins at the level of the disc margin. They are normally present and seen in 37-90% of normals -- depending on the experience of the examiner and the shape of the disc. The spontaneo... | Image |
| 5 |
 |
2-53b - Venous Pulsations | On the disc, look for spontaneous venous pulsations. Spontaneous venous pulsations can be seen in the large trunks of veins at the level of the disc margin. They are normally present and seen in 37-90% of normals -- depending on the experience of the examiner and the shape of the disc. The spontaneo... | Image |
| 6 |
 |
2-6a - Little Red Discs | Image | |
| 7 |
 |
2-6b - Little Red Discs | Image | |
| 8 |
 |
2-7a - Disc Anatomy | The optic disc appearance is determined by: the size of the eye, the size of the scleral canal, how the nerve is inserted into the globe, the appearance of the lamina cribrosa, where myelination stops, and what is left behind in normal development. Even though this is a disc with a very large cup, i... | Image |
| 9 |
 |
3-3 - Bergmeister Papilla | Image | |
| 10 |
 |
3-31b - Papilledema Stages | Grading Papilledema: Stage 0 GRADING PAPILLEDEMA GRADING PAPILLEDEMA We grade papilledema in order to tell us how severe it is. The most sensible grading scheme has been provided by Lars Frisén. STAGE 0: This woman had documented increased intracranial pressure of 340 mm water. Very little if any ... | Image |
| 11 |
 |
3-32b - Papilledema Stages | Grading Papilledema: Stage 1 Stage 1 = C shaped blurring of the nasal, superior and inferior borders. Usually the temporal margin is normal. Also notice the chorio-retinal folds (arrows) that eminate toward the macula (m) | Image |
| 12 |
 |
3-33b - Papilledema Stages | Grading Papilledema: Stage 2 = Elevation of the disc margin 360 degrees. Since the blood vessels at the disc margin are not swollen or obscured, this disc could be mistaken for pseudo-papilledema. | Image |
| 13 |
 |
3-34c Papilledema Stages | Grading Papilledema: Stage 3 Stage 3 = Elevation of the entire disc with partial obscuration of the retinal vessels at the disc margin. Here the vessels are partly obscured and make the development into stage 3 easier to call. | Image |
| 14 |
 |
3-35a - Papilledema Stages | Grading Papilledema: Stage 4 Stage 4 = Complete obliteration of the cup and complete obscuration of at least some vessels on the surface of the disc. There may be small dilated capillaries on the disc that resemble telangiectasia. It is not the NFL infarcts or hemorrhages but the obscuration of the ... | Image |
| 15 |
 |
3-36a - Papilledema Stages | Grading Papilledema: Stage 5 Stage 5 = Dome-shaped appearance with all vessels being obscured. (Sometimes called "champagne cork" swelling--because of its dome shape.) | Image |
| 16 |
 |
3-4 - Tilted Disc | Tilted discs are normal variants caused by oblique insertion of the optic nerve to the globe. They can be and frequently are mistaken for papilledema. In this case the superior edge of the disc is tilted and appears elevated. This disc exhibits a nasal inferior tilt. | Image |
| 17 |
 |
3-56a - Sarcoid | Image | |
| 18 |
 |
3-59a - Glioma | This 45-year-old man presented with vision loss in his right eye; his examination showed severe disc swelling in this eye and vision loss on visual field testing (3-59a). MRI with fat saturation and enhancement and MRI with T2 signals also confirm an enlarged optic nerve. (3-59c) Excisional biopsy o... | Image |
| 19 |
 |
3-59c - Glioma | This 45-year-old man presented with vision loss in his right eye; his examination showed severe disc swelling in this eye and vision loss on visual field testing (3-59a). MRI with fat saturation and enhancement and MRI with T2 signals also confirm an enlarged optic nerve. (3-59c) Excisional biopsy o... | Image |
| 20 |
 |
3-5b - Myelinated Nerve Fibers | Myelinated nerve fibers are frequently confused with papilledema. The feathery edge of the myelinated fibers that conceal the disc and vessel should provide the clue. These myelinated nerve fibers make the disc look blurred. | Image |
| 21 |
 |
3-60a - Meningioma | This 35 year old woman presented with slowly progressive loss of central acuity to 20/30. 3-60a: Her visual field shows progressive restriction over time. 3-60b: Her disc was chronically swollen, with refractile bodies on the disc surface. 3-60d: The CT axial scan showed an enlarged calcified optic... | Image |
| 22 |
 |
3-60b - Meningioma | This 35 year old woman presented with slowly progressive loss of central acuity to 20/30. 3-60a: Her visual field shows progressive restriction over time. 3-60b: Her disc was chronically swollen, with refractile bodies on the disc surface. 3-60d: The CT axial scan showed an enlarged calcified optic... | Image |
| 23 |
 |
3-60d - Meningioma | This 35 year old woman presented with slowly progressive loss of central acuity to 20/30. 3-60a: Her visual field shows progressive restriction over time. 3-60b: Her disc was chronically swollen, with refractile bodies on the disc surface. 3-60d: The CT axial scan showed an enlarged calcified optic... | Image |
| 24 |
 |
3-64a - Shunt Vessels (CRVO) | This man with a chronic CRVO and retino-choroidal collaterals developed AION and his collaterals disappeared. CRVO with retinochoroidal collaterals is almost always associated with multiple peripheral dot and blot hemorrhages as well as nerve fiber layer infarcts of various ages. Notice the retino-c... | Image |
| 25 |
 |
3-65 - Shunt Vessels (Glaucoma) | Chronic end-stage glaucoma produces high pressure that interferes with venous drainage from the disc and broad smooth venous collaterals drain the disc centrifugally to the disc margin where they drain. | Image |
| 26 |
 |
3-66a - Shunt Vessels (Post-papilledema) | The retino-choroidal collaterals seen with chronic papilledema begin with a "Hairnet" of telangiectasias that gradually winnow down to one or more large collateral tortuous draining channel. The presence of these vessels is evidence of long standing disc swelling. When the CSF pressure is lowered, t... | Image |
| 27 |
 |
3-66d - Shunt Vessels (Post-papilledema) | The retino-choroidal collaterals seen with chronic papilledema begin with a "Hairnet" of telangiectasias that gradually winnow down to one or more large collateral tortuous draining channel. The presence of these vessels is evidence of long standing disc swelling. When the CSF pressure is lowered, t... | Image |
| 28 |
 |
4-35 - Cupped Optic Nerve | Atrophic Glaucoma Atrophic glaucomatous discs show thinning of the neuro-retinal rim, "saucerization" (which is shallow cupping), evidence of peripapillary atrophy, and pallor of the very narrow neuroretinal rim. Notice that there is severe atrophy of the nerve fiber layer. | Image |
| 29 |
 |
4-52b - Dominant Optic Neuropathy | A son presented with bilateral optic atrophy of unknown etiology after he failed a school visual exam. When looking for dominant optic atrophy, look at the parents. Mother was examined to find similar kind of atrophy. 4-52a mother, 4-52b son. | Image |
| 30 |
 |
4-54a -Optic Neuropathy, Ischemic: Posterior | Image | |
| 31 |
 |
4-54b - Optic Neuropathy, Ischemic: Posterior | Image | |
| 32 |
 |
4-60a - Dominant Optic Neuropathy | A son presented with bilateral optic atrophy of unknown etiology after he failed a school visual exam. When looking for dominant optic atrophy, look at the parents. Mother was examined to find similar kind of atrophy. 4-60a mother, 4-60b son. | Image |
| 33 |
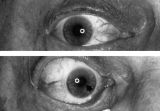 |
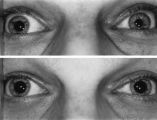
Aberrant Regeneration of the Right Pupil | Aberrant regeneration of the right pupil in a man with a large intracavernous sinus meningioma causing a pupil-involving, incomplete third cranial nerve palsy. His pupil is round when he gazes straight ahead (top). When he tries to rotate the eye medially, the pupil constricts, but a segment of the ... | Image |
| 34 |
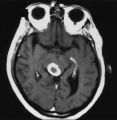 |
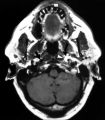
An Enhancing Bladder Metastasis Involving the Tectum of the Midbrain | Magnetic resonance image of an enhancing bladder metastasis involving the tectum of the midbrain of a 56-year-old man who developed double vision resulting from skew deviation and divergence insufficiency. He also had a left-sided relative afferent pupillary defect measuring 1.4 log units but showed... | Image |
| 35 |
 |
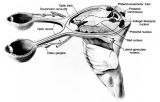
Anatomy of the Oculosympathetic Pathway | Anatomy of the oculosympathetic pathway. (Maloney WF, Younge BR, Moyer NJ: Evaluation of the causes and accuracy of pharmacologic localization in Horner's syndrome. Am J Ophthalmol 1980;90:394-402, Ophthalmic Publishing Company with permission.) | Image |
| 36 |
 |
Anatomy of the Pupillary Light Reflex Pathway | Anatomy of the pupillary light reflex pathway. (Miller NR: Walsh And Hoyt's Clinical Neuro-Ophthalmology, p 421. Vol 2, 4th ed. Baltimore: Williams & Wilkins, 1985, with permission.) | Image |
| 37 |
 |
Argyll Robertson Pupils | Argyll Robertson pupils in an elderly man treated for tabes dorsalis in 1952. His pupils are small and slightly irregular, constrict poorly in response to light stimulation (top), dilate poorly in darkness (middle), but constrict promptly in response to near stimulation (bottom). | Image |
| 38 |
 |
Assessment of an Afferent Pupillary Defect When Only One Iris is Functional | Assessment of an afferent pupillary defect when only one iris is functional. In this example, a right-sided parasellar tumor is compressing both the optic and oculomotor nerves, causing an optic neuropathy and a pupil-involving third crainial nerve palsy. The pupil on the affected side has both an a... | Image |
| 39 |
 |
Bilateral Iris Colobomas | Coloboma literally means a "gap"-and can be used to describe any fissure, hole, or gap in the eye. The term most often is used to refer to a congenital gap in the disc, retina, the choroid, and the iris. Colobomas occur because the embryonic fissure fails to fuse. Since the fissure closure begins in... | Image |
| 40 |
 |
Bilateral Iris Colobomas (B) | Bilateral iris colobomas. B. Bilateral colobomatous defects of the inferonasal retina (black arrows) are also present, as shown in the right eye. | Image |
| 41 |
 |
The Course of the Postganglionic Segment of the Oculosympathetic Fibers from the Internal Carotid Artery | The course of the postganglionic segment of the oculosympathetic fibers from the internal carotid artery (ICA) to the orbit is depicted as a dotted line. Note that they briefly join the abducens nerve (cranial nerve VI) before joining the nasociliary branch of the of the ophthalmic division of the t... | Image |
| 42 |
 |
Enhanced Mydriasis in Response to Hydroxyamphetamine | Enhanced mydriasis in response to hydroxyamphetamine in a 77-year-old woman with a long-standing, preganglionic, right-sided Horner's syndrome that occurred following cervical neck dissection for thoracic outlet syndrome 30 years earlier. Miosis of the right pupil is apparent in room light (top). Th... | Image |
| 43 |
 |
Flow Chart for Sorting Out Anisocoria - Bright Light and Darkness | Flow chart for sorting out anisocoria based initially on how it is influenced by bright light and darkness. | Image |
| 44 |
 |
Flow Chart for Sorting Out Anisocoria - Direct Light Reaction of the Pupil | Flow chart for sorting out anisocoria based initially on the integrity of the direct light reaction of the pupil. | Image |
| 45 |
 |
Hand-held Equipment Used to Measure a Relative Afferent Pupillary Defect | Hand-held equipment used to measure a relative afferent pupillary defect and to record pupil sizes. Four neutral density filters (0.3, 0.6, 0.9, 1.2 log units) are conveniently carried in a soft cloth carrying pouch. A bright light source (a Finhoff model illuminator is shown here) is ideal for stim... | Image |
| 46 |
 |
Left-sided Dilation Lag in a Man with Horner's Syndrome | Left-sided dilation lag in a 29-year-old man with Horner's syndrome caused by a posterior mediastinal ganglioneuroma. Note that the degree of anisocoria is greater after 5 seconds in darkness (top) compared with findings after 15 seconds in darkness (bottom). | Image |
| 47 |
 |
Left-sided Horner's Syndrome with an Acquired Preganglionic Localization | Left-sided Horner's syndrome in a 12-year-old girl with an acquired preganglionic localization based on clinical and pharmacologic testing. The cause remained undetermined after extensive radiologic investigations. Left-sided ptosis and miosis are evident in room light (top), and the degree of aniso... | Image |
| 48 |
 |
Left-sided Internal Carotid Artery Dissection | Left-sided internal carotid artery dissection identified on T-1 weighted magnetic resonance image from a 52-year-old man who suddenly developed left-sided neck and orbital pain along with a droopy left upper eyelid while dragging a deer out of the woods during hunting season. The normal dark flow vo... | Image |
| 49 |
 |
Light-near Dissociation | Light-near dissociation in a 51-year-old woman with multiple sclerosis who experienced double vision for 1 week. Her pupils are 5 mm in diameter in room light (top), react poorly in response to direct light reaction (middle), but constrict promptly in response to near stimulation (bottom). She also ... | Image |
| 50 |
 |
Location of Pupillomotor Fibers | Location of pupillomotor fibers are depicted as dark regions on cross-sections of the right (R) and left (L) oculomotor nerve at various locations along its course, including its emergence from the brain stem in the interpeduncular fossa (1), the midsubarachnoid segment (2), the level of the dorsum ... | Image |