The Health Education Assets Library (HEAL) is a collection of over 22,000 freely available digital materials for health sciences education. The collection is now housed at the University of Utah J. Willard Marriott Digital Library.
TO
| Title | Description | Subject | Collection | ||
|---|---|---|---|---|---|
| 51 |
 |
Complete AV block, junctional escape rhythm, and ventriculophasic sinus arrhythmia | Complete AV block is seen as evidenced by the AV dissociation. A junctional escape rhythm sets the ventricular rate at 45 bpm. The PP intervals vary because of ventriculophasic sinus arrhythmia; this is defined when the PP interval that includes a QRS is shorter than a PP interval that excludes a ... | Knowledge Weavers ECG | |
| 52 |
 |
Junctional parasystole and pseudo-AV block | This complicated rhythm strip shows normal sinus rhythm and a competing junctional parasystolic focus. Solid circles indicate junctional premature beats from the parasystolic focus. Open circles indicate non-conducted junctional prematures; the first open circle is a nonconducted junctional prematur... | Knowledge Weavers ECG | |
| 53 |
 |
Premature junctional complexes with retrograde P waves | The ladder diagram illustrates the PJC with retrograde atrial capture | Knowledge Weavers ECG | |
| 54 |
 |
Left Atrial Abnormality & 1st Degree AV Block: Leads II and V1 | Left Atrial Abnormality & 1st Degree AV Block: Leads II and V1 | Knowledge Weavers ECG | |
| 55 |
 |
Right Axis Deviation & RAE (P pulmonale): Leads I, II, III | Right Axis Deviation & RAE (P pulmonale): Leads I, II, III | Knowledge Weavers ECG | |
| 56 |
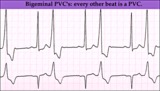 |
Ventricular bigeminy - marquette | Ventricular bigeminy - marquette | Knowledge Weavers ECG | |
| 57 |
 |
LBBB and 2nd degree AV block, mobitz type I | Mobitz II 2nd degree AV block is usually a sign of bilateral bundle branch disease. One of the two bundle branches should be completely blocked; in this example the left bundle is blocked. The nonconducted sinus P waves are most likely blocked in the right bundle which exhibits 2nd degree block. ... | Knowledge Weavers ECG | |
| 58 |
 |
Infero-posterior MI&RBBB | Deep Q waves in II, III, aVF plus tall R waves in V1-2 are evidence for this infero-posterior MI. The wide QRS (>0.12s) and RR' complex in V1 are evidence for RBBB. Any time RBBB has an initial R in V1 equal to or greater than the R', true posterior MI must be considered. Q waves in V5-6 suggest a... | Knowledge Weavers ECG | |
| 59 |
 |
Extensive anterior/anterolateral MI: recent | Significant pathologic Q-waves (V2-6, I, aVL) plus marked ST segment elevation are evidence for this large anterior/anterolateral MI. The exact age of the infarction cannot be determined without clinical correlation and previous ECGs, but this is likely a recent MI. | Knowledge Weavers ECG | |
| 60 |
 |
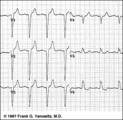
Nonconducted PAC's slowing the heart rate | Consecutive nonconducted PAC's, indicated by arrows, can significantly slow the heart rate. Note the distortion of the ST-T waves caused by the PAC. A hint in recognizing nonconducted PAC's is to find conducted PAC's in the same rhythm strip. | Knowledge Weavers ECG | |
| 61 |
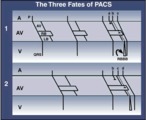 |
three fates of PAC's: 1. normal conduction; 2. aberrant conduction; 3. non-conduction | three fates of PAC's: 1. normal conduction; 2. aberrant conduction; 3. non-conduction | Knowledge Weavers ECG | |
| 62 |
 |
QRS axis = 0 degrees | Lead aVF is isoelectric; lead I is positive; therefore, the QRS axis is 0 degrees. | Knowledge Weavers ECG | |
| 63 |
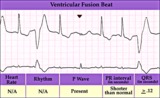 |
Ventricular fusion beat - marquette | Ventricular fusion beat - marquette | Knowledge Weavers ECG | |
| 64 |
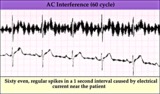 |
60 cycle artifact - marquette | 60 cycle artifact - marquette | Knowledge Weavers ECG | |
| 65 |
 |
LBBB: precordial leads | LBBB: precordial leads | Knowledge Weavers ECG | |
| 66 |
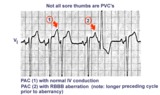 |
Not all sore thumbs are ventricular in origin | PACs have three fates: normal conduction into ventricles, aberrant conduction in ventricles due to bundle branch or fascicular block, and non-conduction due to block in AV junction. In this example PAC 1 is normally conducted and PAC 2 is conducted with RBBB aberration. The longer preceding cycle ... | Knowledge Weavers ECG | |
| 67 |
 |
Acute infero-postero-lateral MI | Hyperacute ST segment elevation is seen in leads II, III, aVF (inferior location) and in leads V4-6 (apical lateral wall location). Hyperacute ST depression is seen in leads V1-2 (an expression of posterior wall injury). in addition there are reciprocal ST segment depression changes in leads I an... | Knowledge Weavers ECG | |
| 68 |
 |
Ventricular Pacemaker Rhythm: V1-3 | Note the small pacemaker spikes before the QRS complexes. In addition, the QRS complex in V1-3 exhibits ventricular ectopic morphology; i.e., there is a slur or notch at the beginning of the S wave, and >60ms delay from onset to QRS to nadir of S wave. This rules against a supraventricular rhythm wi... | Knowledge Weavers ECG | |
| 69 |
 |
Inferior MI: fully evolved | Significant pathologic Q-waves are seen in leads II, III, aVF along with resolving ST segment elevation and symmetrical T wave inversion. This is a classic inferior MI. | Knowledge Weavers ECG | |
| 70 |
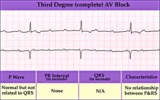 |
Complete AV block (3rd degree) with junctional rhythm | Complete AV block (3rd degree) with junctional rhythm | Knowledge Weavers ECG | |
| 71 |
 |
QRS axis = +90 degrees | Lead I is isoelectric; II and III are positive; the axis is +90 degrees. | Knowledge Weavers ECG | |
| 72 |
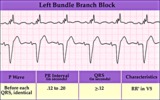 |
Left bundle branch block - marquette | Left bundle branch block - marquette | Knowledge Weavers ECG | |
| 73 |
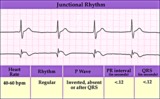 |
Junctional escape rhythm | Junctional escape rhythm | Knowledge Weavers ECG | |
| 74 |
 |
Diagram: AV nodal reentrant tachycardia | The AV node often has dual pathways; in this diagram the alpha pathway is fast, but has a long refractory period; the beta pathway is conducts more slowly, but recovers faster.In sinus rhythm the faster alpha pathway is used and accounts for the normal PR interval. When a PAC occurs, however, the i... | Knowledge Weavers ECG | |
| 75 |
 |
Atrial parasystole | In atrial parasystole non-fixed coupled PACs, shown by arrows, occur at a common inter-ectopic interval or at multiples of this interval. Atrial fusions, not shown here, may also occur when the PAC occurs in close temporal proximity to the sinus impulse. | Knowledge Weavers ECG |