John A. Moran Eye Center Neuro-Ophthalmology Collection: A variety of lectures, videos and images relating to topics in Neuro-Ophthalmology created by faculty at the Moran Eye Center, University of Utah, in Salt Lake City.
NOVEL: https://novel.utah.edu/
TO
1 - 200 of 196
| Title | Description | Type | ||
|---|---|---|---|---|
| 1 |
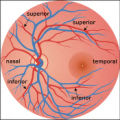 |
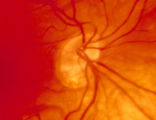
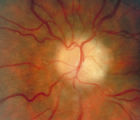
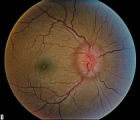
2-37a - Vascular Features | When looking at the disc, the central retinal artery and vein should be visible. The central retinal artery is usually slightly narrower than the vein. When the central retinal artery goes though the lamina cribrosa, the artery becomes smaller because of diminution of the muscular layer and loss of ... | Image |
| 2 |
 |
2-37b - Vascular Features | When looking at the disc, the central retinal artery and vein should be visible. The central retinal artery is usually slightly narrower than the vein. When the central retinal artery goes though the lamina cribrosa, the artery becomes smaller because of diminution of the muscular layer and loss of ... | Image |
| 3 |
 |
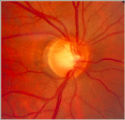
2-4a - Disc Anatomy | The optic disc appearance is determined by: the size of the eye, the size of the scleral canal, how the nerve is inserted into the globe, the appearance of the lamina cribrosa, where myelination stops, and what is left behind in normal development. Even though this is a disc with a very large cup, i... | Image |
| 4 |
 |
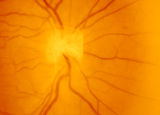
2-53a - Venous Pulsations | On the disc, look for spontaneous venous pulsations. Spontaneous venous pulsations can be seen in the large trunks of veins at the level of the disc margin. They are normally present and seen in 37-90% of normals -- depending on the experience of the examiner and the shape of the disc. The spontaneo... | Image |
| 5 |
 |
2-53b - Venous Pulsations | On the disc, look for spontaneous venous pulsations. Spontaneous venous pulsations can be seen in the large trunks of veins at the level of the disc margin. They are normally present and seen in 37-90% of normals -- depending on the experience of the examiner and the shape of the disc. The spontaneo... | Image |
| 6 |
 |
2-6a - Little Red Discs | Image | |
| 7 |
 |
2-6b - Little Red Discs | Image | |
| 8 |
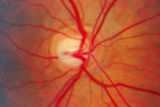 |
2-7a - Disc Anatomy | The optic disc appearance is determined by: the size of the eye, the size of the scleral canal, how the nerve is inserted into the globe, the appearance of the lamina cribrosa, where myelination stops, and what is left behind in normal development. Even though this is a disc with a very large cup, i... | Image |
| 9 |
 |
3 Step Test | Demonstration of patient examination. | Image/MovingImage |
| 10 |
 |
3-3 - Bergmeister Papilla | Image | |
| 11 |
 |
3-31b - Papilledema Stages | Grading Papilledema: Stage 0 GRADING PAPILLEDEMA GRADING PAPILLEDEMA We grade papilledema in order to tell us how severe it is. The most sensible grading scheme has been provided by Lars Frisén. STAGE 0: This woman had documented increased intracranial pressure of 340 mm water. Very little if any ... | Image |
| 12 |
 |
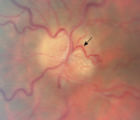
3-32b - Papilledema Stages | Grading Papilledema: Stage 1 Stage 1 = C shaped blurring of the nasal, superior and inferior borders. Usually the temporal margin is normal. Also notice the chorio-retinal folds (arrows) that eminate toward the macula (m) | Image |
| 13 |
 |
3-33b - Papilledema Stages | Grading Papilledema: Stage 2 = Elevation of the disc margin 360 degrees. Since the blood vessels at the disc margin are not swollen or obscured, this disc could be mistaken for pseudo-papilledema. | Image |
| 14 |
 |
3-34c Papilledema Stages | Grading Papilledema: Stage 3 Stage 3 = Elevation of the entire disc with partial obscuration of the retinal vessels at the disc margin. Here the vessels are partly obscured and make the development into stage 3 easier to call. | Image |
| 15 |
 |
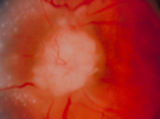
3-35a - Papilledema Stages | Grading Papilledema: Stage 4 Stage 4 = Complete obliteration of the cup and complete obscuration of at least some vessels on the surface of the disc. There may be small dilated capillaries on the disc that resemble telangiectasia. It is not the NFL infarcts or hemorrhages but the obscuration of the ... | Image |
| 16 |
 |
3-36a - Papilledema Stages | Grading Papilledema: Stage 5 Stage 5 = Dome-shaped appearance with all vessels being obscured. (Sometimes called "champagne cork" swelling--because of its dome shape.) | Image |
| 17 |
 |
3-4 - Tilted Disc | Tilted discs are normal variants caused by oblique insertion of the optic nerve to the globe. They can be and frequently are mistaken for papilledema. In this case the superior edge of the disc is tilted and appears elevated. This disc exhibits a nasal inferior tilt. | Image |
| 18 |
 |
3-56a - Sarcoid | Image | |
| 19 |
 |
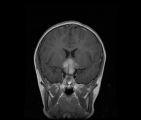
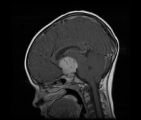
3-59a - Glioma | This 45-year-old man presented with vision loss in his right eye; his examination showed severe disc swelling in this eye and vision loss on visual field testing (3-59a). MRI with fat saturation and enhancement and MRI with T2 signals also confirm an enlarged optic nerve. (3-59c) Excisional biopsy o... | Image |
| 20 |
 |
3-59c - Glioma | This 45-year-old man presented with vision loss in his right eye; his examination showed severe disc swelling in this eye and vision loss on visual field testing (3-59a). MRI with fat saturation and enhancement and MRI with T2 signals also confirm an enlarged optic nerve. (3-59c) Excisional biopsy o... | Image |
| 21 |
 |
3-5b - Myelinated Nerve Fibers | Myelinated nerve fibers are frequently confused with papilledema. The feathery edge of the myelinated fibers that conceal the disc and vessel should provide the clue. These myelinated nerve fibers make the disc look blurred. | Image |
| 22 |
 |
3-60a - Meningioma | This 35 year old woman presented with slowly progressive loss of central acuity to 20/30. 3-60a: Her visual field shows progressive restriction over time. 3-60b: Her disc was chronically swollen, with refractile bodies on the disc surface. 3-60d: The CT axial scan showed an enlarged calcified optic... | Image |
| 23 |
 |
3-60b - Meningioma | This 35 year old woman presented with slowly progressive loss of central acuity to 20/30. 3-60a: Her visual field shows progressive restriction over time. 3-60b: Her disc was chronically swollen, with refractile bodies on the disc surface. 3-60d: The CT axial scan showed an enlarged calcified optic... | Image |
| 24 |
 |
3-60d - Meningioma | This 35 year old woman presented with slowly progressive loss of central acuity to 20/30. 3-60a: Her visual field shows progressive restriction over time. 3-60b: Her disc was chronically swollen, with refractile bodies on the disc surface. 3-60d: The CT axial scan showed an enlarged calcified optic... | Image |
| 25 |
 |
3-64a - Shunt Vessels (CRVO) | This man with a chronic CRVO and retino-choroidal collaterals developed AION and his collaterals disappeared. CRVO with retinochoroidal collaterals is almost always associated with multiple peripheral dot and blot hemorrhages as well as nerve fiber layer infarcts of various ages. Notice the retino-c... | Image |
| 26 |
 |
3-65 - Shunt Vessels (Glaucoma) | Chronic end-stage glaucoma produces high pressure that interferes with venous drainage from the disc and broad smooth venous collaterals drain the disc centrifugally to the disc margin where they drain. | Image |
| 27 |
 |
3-66a - Shunt Vessels (Post-papilledema) | The retino-choroidal collaterals seen with chronic papilledema begin with a "Hairnet" of telangiectasias that gradually winnow down to one or more large collateral tortuous draining channel. The presence of these vessels is evidence of long standing disc swelling. When the CSF pressure is lowered, t... | Image |
| 28 |
 |
3-66d - Shunt Vessels (Post-papilledema) | The retino-choroidal collaterals seen with chronic papilledema begin with a "Hairnet" of telangiectasias that gradually winnow down to one or more large collateral tortuous draining channel. The presence of these vessels is evidence of long standing disc swelling. When the CSF pressure is lowered, t... | Image |
| 29 |
 |
4-35 - Cupped Optic Nerve | Atrophic Glaucoma Atrophic glaucomatous discs show thinning of the neuro-retinal rim, "saucerization" (which is shallow cupping), evidence of peripapillary atrophy, and pallor of the very narrow neuroretinal rim. Notice that there is severe atrophy of the nerve fiber layer. | Image |
| 30 |
 |
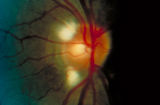
4-52b - Dominant Optic Neuropathy | A son presented with bilateral optic atrophy of unknown etiology after he failed a school visual exam. When looking for dominant optic atrophy, look at the parents. Mother was examined to find similar kind of atrophy. 4-52a mother, 4-52b son. | Image |
| 31 |
 |
4-54a -Optic Neuropathy, Ischemic: Posterior | Image | |
| 32 |
 |
4-54b - Optic Neuropathy, Ischemic: Posterior | Image | |
| 33 |
 |
4-60a - Dominant Optic Neuropathy | A son presented with bilateral optic atrophy of unknown etiology after he failed a school visual exam. When looking for dominant optic atrophy, look at the parents. Mother was examined to find similar kind of atrophy. 4-60a mother, 4-60b son. | Image |
| 34 |
 |
Abducting (Dissociated) Nystagmus | Example of a patient with abducting (dissociated) nystagmus. Patient has a subtle internuclear ophthalmoplegia. Right eye has right-beating jerk nystagmus, with smaller oscillations in the left eye. Disease/Diagnosis: Abducting Nystagmus | Image/MovingImage |
| 35 |
 |
Aberrant Regeneration of the Lid | Patient with left third nerve palsy demonstrates anisocoria and mild vertical gaze limitation and aberrant movement of the left upper lid. Patient is instructed through all gaze positions. Left upper lid does not descend during downgaze but retracts instead. | Image/MovingImage |
| 36 |
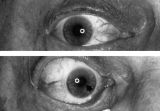 |
Aberrant Regeneration of the Right Pupil | Aberrant regeneration of the right pupil in a man with a large intracavernous sinus meningioma causing a pupil-involving, incomplete third cranial nerve palsy. His pupil is round when he gazes straight ahead (top). When he tries to rotate the eye medially, the pupil constricts, but a segment of the ... | Image |
| 37 |
 |
Aberrant Regeneration of the Seventh Nerve | Examples of patients with aberrant regeneration of the seventh nerve. First example is a patient with contractions around the mouth and dimpling, demonstrated with slow and rapid eye blinking. Second example shows contraction around nose with eye blink. | Image/MovingImage |
| 38 |
 |
Aberrant Regeneration of the Third | Patient with a right third nerve palsy demonstrates ptosis, anisocoria and ophthalmoplegia. During attempted downgaze, the right upper lid flutters back up (aberrant movement) and remains retracted. | Image/MovingImage |
| 39 |
 |
Aberrant Regeneration of the Third and Sixth Nerves | Image/MovingImage | |
| 40 |
|
Aberrant Regeneration of Third Nerve, Bilaterally (1 degree OD, 2 Digrees OS) | Example of patient with bilateral aberrancy of the third nerve. Shows lids popping up (synkinetic) with adduction. Patient had bilateral internal carotid artery aneurisms with third nerve compression. | Image/MovingImage |
| 41 |
 |
Amsler Grid Testing | Demonstration of Amsler Grid examination. | Text |
| 42 |
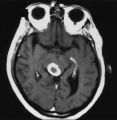 |
An Enhancing Bladder Metastasis Involving the Tectum of the Midbrain | Magnetic resonance image of an enhancing bladder metastasis involving the tectum of the midbrain of a 56-year-old man who developed double vision resulting from skew deviation and divergence insufficiency. He also had a left-sided relative afferent pupillary defect measuring 1.4 log units but showed... | Image |
| 43 |
 |
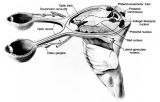
Anatomy of the Oculosympathetic Pathway | Anatomy of the oculosympathetic pathway. (Maloney WF, Younge BR, Moyer NJ: Evaluation of the causes and accuracy of pharmacologic localization in Horner's syndrome. Am J Ophthalmol 1980;90:394-402, Ophthalmic Publishing Company with permission.) | Image |
| 44 |
 |
Anatomy of the Pupillary Light Reflex Pathway | Anatomy of the pupillary light reflex pathway. (Miller NR: Walsh And Hoyt's Clinical Neuro-Ophthalmology, p 421. Vol 2, 4th ed. Baltimore: Williams & Wilkins, 1985, with permission.) | Image |
| 45 |
 |
Anterior Ischemic Optic Neuropathy | PPT describing Anterior Ischemic Optic Neuropathy (AION). Covers clinical signs, such as monocular vision loss, swollen nerve, and visual field defects, as well as risk factors. | Text |
| 46 |
 |
Argyll Robertson Pupils | Argyll Robertson pupils in an elderly man treated for tabes dorsalis in 1952. His pupils are small and slightly irregular, constrict poorly in response to light stimulation (top), dilate poorly in darkness (middle), but constrict promptly in response to near stimulation (bottom). | Image |
| 47 |
 |
Assessment of an Afferent Pupillary Defect When Only One Iris is Functional | Assessment of an afferent pupillary defect when only one iris is functional. In this example, a right-sided parasellar tumor is compressing both the optic and oculomotor nerves, causing an optic neuropathy and a pupil-involving third crainial nerve palsy. The pupil on the affected side has both an a... | Image |
| 48 |
 |
Basal Encephaloceles | Text | |
| 49 |
 |
Basic Eye Alignment Exam | Demonstration of basic eye alignment examination. Includes: a. Tools b. Cover-Uncover and SPCT c. Alternate Cover and APCT d. Maddox Rod Testing | Image/MovingImage |
| 50 |
 |
Before Tensilon | Example of patient with myasthenia gravis. Demonstration of baseline examination, followed by administration of 2mg of tensilon, which is a test dose. Procedure for administration of tensilon test is described, including variations. Patient is then shown after being given 4mg of tensilon, with very ... | Image/MovingImage |
| 51 |
 |
Bilateral Asynchronous Blepharospasm with Facial and Cervical Dystonia | Bilateral Asynchronous Blepharospasm with Facial and Cervical Dystonia. | Image/MovingImage |
| 52 |
 |
Bilateral Facial Myokymia | Example of a patient with a brain stem glioma. Shows bilateral facial myokymia. | Image/MovingImage |
| 53 |
 |
Bilateral Internuclear Ophthalmoplegia | Example of patient with bilateral internuclear ophthalmoplegia. Patient is led through instructions for direction and distance of gaze. | Image/MovingImage |
| 54 |
 |
Bilateral Iris Colobomas | Coloboma literally means a "gap"-and can be used to describe any fissure, hole, or gap in the eye. The term most often is used to refer to a congenital gap in the disc, retina, the choroid, and the iris. Colobomas occur because the embryonic fissure fails to fuse. Since the fissure closure begins in... | Image |
| 55 |
 |
Bilateral Iris Colobomas (B) | Bilateral iris colobomas. B. Bilateral colobomatous defects of the inferonasal retina (black arrows) are also present, as shown in the right eye. | Image |
| 56 |
 |
Bilateral Ptosis | Video of patient with bilateral ptosis. | Image/MovingImage |
| 57 |
 |
Binocular Pendular Nystagmus | Example of a patient with binocular pendular nystagmus. Patient has somewhat dissociated nystagmus, with nystagmus seen more prominently in the left eye. Patient shows an occasional jerk nystagmus to the right in the right eye. Left eye oscillations are mostly pendular. | Image/MovingImage |
| 58 |
 |
Blepharospasm | Example of patient with blepharospasm. Patient is led through instructions for direction of gaze and opening and closing of eyes. Patient is led through same exercises again after receiving indomethacin treatment. | Image/MovingImage |
| 59 |
 |
Blepharospasm with Apraxia of the Eye | Image/MovingImage | |
| 60 |
 |
Brainstem Trauma | Image/MovingImage | |
| 61 |
 |
Brun's Nystagmus | Observation of patient with Brun's Nystagmus. Shows patient gazing to the right and the nystagmus beating in the direction of the gaze. | Image/MovingImage |
| 62 |
 |
Central Retinal Artery Occlusion | Video of central retinal artery occlusion. | Image/MovingImage |
| 63 |
 |
Cogan's Lid Twitch | Image/MovingImage | |
| 64 |
 |
Cogan's Lid Twitch | Example of a patient with Cogan's lid twitch, with discussion of how to detect it in an exam. | Image/MovingImage |
| 65 |
 |
Color Vision Testing | Demonstration of color vision examination. | Text |
| 66 |
 |
Cone Dystrophy | PPT covering Cone Dystrophy - An inherited degeneration that presents between 10 - 30 years of age. Symptoms are decreased visual acuity, poor color vision, and sometimes light sensitivity. | Text |
| 67 |
 |
Congenital Nystagmus | Example of patients with congenital nystagmus. First patient's nystagmus are mostly jerk and not pendular. Second patient's nystagmus are mostly pendular. Both patients show a uniform horizontal oscillation. Second patient also shows differences in frequency of oscillations depending on gaze, includ... | Image/MovingImage |
| 68 |
 |
Congenital Nystagmus | Patient with congenital nystagmus (no audio) | Image/MovingImage |
| 69 |
 |
Congenital Ocular Motor Apraxia | Two examples of congenital ocular motor apraxia. Patients have trouble initiating saccades, and compensate with head movement. Discussion of how to distinguish this condition from simply not seeing well. | Image/MovingImage |
| 70 |
 |
Convergence Retraction Nystagmus (Parinaud's Syndrome) | Examples of patients with convergence retraction nystagmus. Shows saccadic oscillations in patients looking upwards and following downwards moving targets. Also shows a side-view of the retracting movements of the globes. | Image/MovingImage |
| 71 |
 |
The Course of the Postganglionic Segment of the Oculosympathetic Fibers from the Internal Carotid Artery | The course of the postganglionic segment of the oculosympathetic fibers from the internal carotid artery (ICA) to the orbit is depicted as a dotted line. Note that they briefly join the abducens nerve (cranial nerve VI) before joining the nasociliary branch of the of the ophthalmic division of the t... | Image |
| 72 |
 |
CPEO | Patient with Chronic Progressive External Ophthalmoplegia (CPEO) | Image/MovingImage |
| 73 |
 |
Cyclic Oculomotor Palsy | Example of patient with cyclic oculomotor palsy. | Image/MovingImage |
| 74 |
 |
Dilation Lag | Two examples of dilation lag (Horner's syndrome). In the first example, the right pupil dilates much faster than the left pupil when the light is turned out. In the second example, the left pupil dilates much faster than the right pupil when the light is turned out. Discussion of methods of document... | Image/MovingImage |
| 75 |
 |
Dissection of the Carotid Artery | ||
| 76 |
 |
Dissociated Nystagmus | Example of a patient with dissociated nystagmus. Demonstrates difference in movements between each eye. | Image/MovingImage |
| 77 |
 |
Downbeat Nystagmus | Example of patients with downbeating jerk nystagmus. Demonstrates how oscillations grow more prominent when the patient gazes down or laterally. Discusses some causes, including Arnold-Chiari malformation, infarction, and demyelination. | Image/MovingImage |
| 78 |
 |
Downbeat Nystagmus | Example of patient with downbeat nystagmus. Patient is led through instructions of where to gaze. (no audio) | Image/MovingImage |
| 79 |
 |
Downbeat Nystagmus | Example of patient with downbeat nystagmus. Patient is led through instructions of where to gaze. | Image/MovingImage |
| 80 |
 |
Duane's Retraction Syndrome Type 1: Lid Retraction | Example of patients with Duane's Retraction Syndrome, Type 1. Description of components of Duane's Syndrome: limitation of abduction, variable limitation of adduction, and palpebral fissure narrowing and globe retraction with attempted adduction. Type 1 includes limited or absent abduction with norm... | Image/MovingImage |
| 81 |
 |
Duane's Retraction Syndrome Type 3 | Example of a patient with Type 3 Duane's Retraction Syndrome, as well as bilateral Duane's Syndrome. Shows limitation of abduction in both eyes and adduction in the left eye. Also shows side-view of globe retraction in abduction. | Image/MovingImage |
| 82 |
 |
Duane's Syndrome | Example of patient with Duane's Syndrome. Patient is led through instructions for pursuit. | Image/MovingImage |
| 83 |
 |
Duane's Syndrome Type 1 | Clip of patient with Duane's Syndrome Type I. Presented at the Neurology Grand Rounds in Fall 2011 at the University of Utah. Presentation can be found in this collection at: Why Don't You See Double? http://content.lib.utah.edu/u?/EHSL-Moran-Neuro-opth,132 Disease/Diagnosis: Duane's Syndrome Type ... | Image/MovingImage |
| 84 |
 |
Duane's Syndrome Type 2: Aberrant Regeneration of the Third and Sixth Nerves | Example of a patient with Type 2 Duane's Syndrome. Demonstrates limitation of adduction in left eye with normal abduction. Discussion of limited pathological cases. | Image/MovingImage |
| 85 |
 |
Duane's Syndrome Type 3 | Clip of patient with Duane's Syndrome Type III. Presented at the Neurology Grand Rounds in Fall 2011 at the University of Utah. Presentation can be found in this collection at: Why Don't You See Double? http://content.lib.utah.edu/u?/EHSL-Moran-Neuro-opth,132 Disease/Diagnosis: Duane's Syndrome Ty... | Image/MovingImage |
| 86 |
 |
Dysthyroid Optic Neuropathy: A Preventable Cause of Blindness | Dysthyroid Optic Neuropathy (DON) is a treatable cause of visual loss in ~5% of pts w/ ted. Monitor closely those pts with risk factors (proptosis, tight orbit, restricted motility, strabismus, smoker, diabetic). Oral prednisone is often effective, but frequent relapses after tapering. Orbital xrt ... | |
| 87 |
 |
Enhanced Mydriasis in Response to Hydroxyamphetamine | Enhanced mydriasis in response to hydroxyamphetamine in a 77-year-old woman with a long-standing, preganglionic, right-sided Horner's syndrome that occurred following cervical neck dissection for thoracic outlet syndrome 30 years earlier. Miosis of the right pupil is apparent in room light (top). Th... | Image |
| 88 |
 |
Facial Myokymia Unilateral | Example of patient with facial myokymia, a disorder of the seventh nerve, probably due to brain stem involvement. Patient has multiple sclerosis. Discussion of characteristics, such as continuous, undulating, contractions in the distribution of the seventh nerve, and a spreading of these movements t... | Image/MovingImage |
| 89 |
 |
Flow Chart for Sorting Out Anisocoria - Bright Light and Darkness | Flow chart for sorting out anisocoria based initially on how it is influenced by bright light and darkness. | Image |
| 90 |
 |
Flow Chart for Sorting Out Anisocoria - Direct Light Reaction of the Pupil | Flow chart for sorting out anisocoria based initially on the integrity of the direct light reaction of the pupil. | Image |
| 91 |
 |
Flutter in Downgaze | Examination of patient with flutter in downgaze (no audio) | Image/MovingImage |
| 92 |
 |
Fourth Nerve Palsy | Demonstration of examination of patient who experienced blurry vision and pain in the left eye. Demonstrates checking of eye movements, focusing on object while each eye is covered and uncovered, turning head both ways and repeating. Shows limitation of depression in adduction of left eye, left hype... | Image/MovingImage |
| 93 |
 |
Fusional Vergence Amplitudes | Demonstration of fusional vergence amplitudes examination. Incluudes: a. Convergence Amplitudes b. Divergence Amplitudes c. Vertical Ampitudes | Text |
| 94 |
 |
Gaze Palsy with Facial Weakness from Pontine AVM | Example of a patient with torsional nystagmus in both eyes and pendular nystagmus in the left eye. Patient is led through instructions for direction of gaze. | Image/MovingImage |
| 95 |
 |
Glaucoma: The Basics | Glaucoma is the most common optic neuropathy. Progressive cupping of the optic disc due to increased intraocular pressure together with visual field abnormalities and local disc susceptibility factors characterize this neuropathy. This PowerPoint lecture covers the basics of Glaucoma and includes ma... | Text |
| 96 |
 |
Hand-held Equipment Used to Measure a Relative Afferent Pupillary Defect | Hand-held equipment used to measure a relative afferent pupillary defect and to record pupil sizes. Four neutral density filters (0.3, 0.6, 0.9, 1.2 log units) are conveniently carried in a soft cloth carrying pouch. A bright light source (a Finhoff model illuminator is shown here) is ideal for stim... | Image |
| 97 |
 |
Hemifacial Spasm | Example of patients with hemifacial spasm. First patient has a sequela of Bell's palsy, and is seen to have mainly clonic movements around the eye, with occasional tonic movements around the mouth. Second patient has a cerebellopontine angle epidurmoid tumor, and is seen to have movements around the... | Image/MovingImage |
| 98 |
 |
Herpes Zoster Ophthalmicus with Third Nerve Palsy | Images showing presentation of Herpes Zoster (Zoster Ophthalmicus). | Text |
| 99 |
 |
How to Measure the RAPD | This clip demonstrates the examination technique for measuring the Relative Afferent Pupillary Defect (RAPD). Demonstration of balancing an afferent papillary defect using filters in a patient with a resolving optic neuritis and an afferent papillary defect on the left. | Image/MovingImage |
| 100 |
 |
How to Use the Direct Ophthalmoscope in an Exam | Demonstration of using the direct ophthalmoscope to examine the optic disc. Covers hand placement , which eye to use, and distance from patient. | Image/MovingImage |
| 101 |
 |
Hydroxychloroquine Maculopathy (Plaquenil) | An overview of Chloroquine Maculopathy. | Text |
| 102 |
 |
Intermittent Square Wave Jerks | Patient with intermittent square wave jerks (no audio) | Image/MovingImage |
| 103 |
 |
Internuclear Ophthalmoplegia (2 Examples) | Two examples of patients with internuclear ophthalmoplegia. First patient has a right internuclear ophthalmoplegia. Patient had subacute bacterial endocarditis with a bacterial abscess in the brain stem. Ductions and gaze to the right look good, but when gazing to the left, the right eye does not ad... | Image/MovingImage |
| 104 |
|
Latent Nystagmus | Example of a patient with latent nystagmus. Demonstrates a lack of oscillations in forward gaze, followed by the occlusion of each eye, showing how this generates a jerking oscillation in the non-occluded eye away from the occluded eye. | Image/MovingImage |
| 105 |
 |
Leber's Hereditary Optic Neuropathy | Images and visual fields from a boy with acute visual loss. | Text |
| 106 |
 |
Left-sided Dilation Lag in a Man with Horner's Syndrome | Left-sided dilation lag in a 29-year-old man with Horner's syndrome caused by a posterior mediastinal ganglioneuroma. Note that the degree of anisocoria is greater after 5 seconds in darkness (top) compared with findings after 15 seconds in darkness (bottom). | Image |
| 107 |
 |
Left-sided Horner's Syndrome with an Acquired Preganglionic Localization | Left-sided Horner's syndrome in a 12-year-old girl with an acquired preganglionic localization based on clinical and pharmacologic testing. The cause remained undetermined after extensive radiologic investigations. Left-sided ptosis and miosis are evident in room light (top), and the degree of aniso... | Image |
| 108 |
 |
Left-sided Internal Carotid Artery Dissection | Left-sided internal carotid artery dissection identified on T-1 weighted magnetic resonance image from a 52-year-old man who suddenly developed left-sided neck and orbital pain along with a droopy left upper eyelid while dragging a deer out of the woods during hunting season. The normal dark flow vo... | Image |
| 109 |
 |
Levator Disinsertion | Example of patient with levator disinsertion, a lid disorder. Patient is pregnant and wears poorly fitting contacts. Discussion of characteristics, such as lid ptosis (shown in the left eye of patient), but with full levator function. | Image/MovingImage |
| 110 |
 |
Light-near Dissociation | Light-near dissociation in a 51-year-old woman with multiple sclerosis who experienced double vision for 1 week. Her pupils are 5 mm in diameter in room light (top), react poorly in response to direct light reaction (middle), but constrict promptly in response to near stimulation (bottom). She also ... | Image |
| 111 |
|
Light-near Dissociation | Example of patient with Argyll Robertson pupil with neurosyphilis. Shows a lack of pupillary response to light and some pupillary response to nearness of finger. | Image/MovingImage |
| 112 |
 |
Location of Pupillomotor Fibers | Location of pupillomotor fibers are depicted as dark regions on cross-sections of the right (R) and left (L) oculomotor nerve at various locations along its course, including its emergence from the brain stem in the interpeduncular fossa (1), the midsubarachnoid segment (2), the level of the dorsum ... | Image |
| 113 |
 |
Macula | Overview of the structure and viewing of the macula. | Text |
| 114 |
 |
Marcus Gunn Jaw Winking | Example of patient with Marcus Jaw Winking. Patient is led through instructions for movement of jaw (open, close, back and forth), with eyelid seen to be affected. Patient is then led through instructions for direction of gaze and pursuit. | Image/MovingImage |
| 115 |
 |
Measuring Visual Acuity | Demonstration on self of visual acuity exam, using a standard card. | Image/MovingImage |
| 116 |
 |
MELAS and RP | MELAS; Mitochondrial Encephalopathy with Lactic Acidosis, Stroke and Pigmentary Changes in retina-associated with a retinal dystrophy. This 53 year old man had seizures, encephalopathy and lactic acidosis typical of MELAS. His fundus examination showed granularity and some slight pigmentary changes ... | Text |
| 117 |
 |
Mimics of Atrophy | Text | |
| 118 |
 |
Monocular Pendular Nystagmus | Example of a patient with monocular pendular nystagmus, with discussion of situations in which this condition is seen: acquired disorder of the visual-sensory pathway, and acquired disorder of the brain stem (e.g. multiple sclerosis). | Image/MovingImage |
| 119 |
 |
Normal Eye Movements | This is an examination of a person with normal eye movements. Notice the patient has normal excursions. He has normal pursuit and saccades (horizontally and vertically). | Text |
| 120 |
 |
Normal Light Reflex without RAPD | This clip demonstrates the examination of the Relative Afferent Pupillary Defect (RAPD.) Demonstration of gauging the size of the pupil in light, testing light reflexes, swinging flashlight test for optic nerve abnormality. | Image/MovingImage |
| 121 |
 |
Normal Optic Disc | Overview of the structure and function of the normal optic disc. | Text |
| 122 |
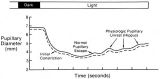 |
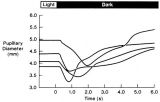
The Normal Pupillary Light Reflex | The normal pupillary light reflex is initiated following exposure to light. After a brief latency, both the right (solid line) and left (broken line) pupil constrict, then undergo a small amount of redilation (escape), followed by oscillations (hippus) if the light is sustained. Hippus is not a path... | Image |
| 123 |
 |
Notching of the Neuro-retinal Rim | The neuro-retinal rim becomes thinner; in particular the rim superotemporally and inferortemporally may develop a notch which is usually superior or inferior and rarely nasal or temporal. These notches are believed to be due to focal ischemic damage to the neuro-retinal rim. Glaucoma with Notching a... | Image |
| 124 |
 |
Nutritional Amblyopia | Example of patient with amblyopia with nutritional causes. | Text |
| 125 |
 |
Ocular Flutter | Two examples of patients, the first with rotary, flutter-like movements, but not ocular flutter, and the second with genuine ocular flutter. Discussion of difference between ocular flutter and nystagmus, and how to elicit ocular flutter. | Image/MovingImage |
| 126 |
|
Ocular Lateropulsion (Wallenberg's Syndrome) | Example of patient with ocular lateropulsion. Patient also has central Horner syndrome and nystagmus in right gaze. When shifting gaze back to forward, eyes overshoot their mark. Eyes laterally deviate to the right upon opening. | Image/MovingImage |
| 127 |
 |
Ocular Myasthenia | Example of patient with myasthenia gravis. Demonstration of tensilon test. Patient shown to have bilateral ptosis, bilateral duction deficits, and left hypertropia. Discussion of techniques to observe subtle changes, such as bringing in a neutral observer or taking still photographs. Shows split-scr... | Image/MovingImage |
| 128 |
 |
Ocular Myotonia | Example of patient with ocular myotonia. Patient is led through instructions for direction of gaze and opening and closing of eyes. Right eye is shown to be stuck in position after held gaze to the left and right, with very slow relaxation back into forward gaze. | Image/MovingImage |
| 129 |
 |
Oculopalatal Myoclonus | Oculopalatal myoclonus (OPM) Rhythmic oscillations of eyes and palate. Occurred after specific brainstem injury from stroke, following stenting. Related PowerPoint Presentation: http://content.lib.utah.edu/u?/EHSL-Moran-Neuro-opth,129 Disease/Diagnosis: Oculopalatal myoclonus. | Image/MovingImage |
| 130 |
 |
Oculopalatal Myoclonus (PPT) | Oculopalatal myoclonus (OPM) Rhythmic oscillations of eyes and palate. Occurred after specific brainstem injury from stroke, following stenting. Related Video: http://content.lib.utah.edu/u?/EHSL-Moran-Neuro-opth,128 Disease/Diagnosis: Oculopalatal myoclonus | Image/MovingImage |
| 131 |
 |
Opsoclonus | Example of patients with opsoclonus, a saccadic abnormality. | Image/MovingImage |
| 132 |
 |
Opsoclonus | Example of patients with opsoclonus, a saccadic abnormality. Discussion of characteristics of opsoclonus, such as involuntary, rapid, brief, random, conjugate saccades. Discussion of possible causes, including brain stem encephalitis (as in first patient), a paraneoplastic effect, tumors, and drug t... | Image/MovingImage |
| 133 |
 |
Optic Disc Pallor Pseudo and Real | Discussion of the causes of optic disc pallor. | Text |
| 134 |
 |
Optic Disc: Anatomy, Variants, Unusual discs | Discussion of viewing the optic disc. Includes development of direct ophthalmoscope. Covers normal optic disc and nerve fiber; nerve fiber loss and defects; cilioretinal arteries; venous anomolies; papilledema; pseudopapilledema; myopic disc; hyperoptic disc; little red discs; megallopapilla; myelin... | Text |
| 135 |
 |
Optic Nerve Tumors Benign and Malignant | Discussion of optic nerve tumors including meningioma and glioma. | Text |
| 136 |
 |
Papilledema 2013 | Discussion of papilledema, the swelling due to increased pressure. | Text |
| 137 |
|
Paradoxical Constriction of Pupils to Darkness (Flynn Phenomenon) | Example of patients both with and without paradoxical constriction of pupils. Observed in many congenital retinal disorders, such as achromatopsia, congenital stationary night-blindness, and Leber's congenital amaurosis. Sometimes seen in optic nerve disorders, such as dominant optic atrophy. | Image/MovingImage |
| 138 |
 |
Parinaud's Syndrome | Two examples of patients with Parinaud's syndrome, a dorsal midbrain syndrome. Discussion of hallmarks of this syndrome, including convergence retraction nystagmus, vertical gaze palsies, light-near dissociation, and Collier's Sign. Discussion of age-dependent disorders associated with this syndrome... | Image/MovingImage |
| 139 |
 |
Pathophysiology of Signs Associated with a Tonic Pupil | Pathophysiology of signs associated with a tonic pupil. Normally, all parasympathetic fibers of the third cranial nerve synapse in the ciliary ganglion (top). Most postganglionic fibers innervate the ciliary muscle (dashed lines). After injury to the ciliary ganglion, the pupil becomes denervated an... | Image |
| 140 |
|
Periodic Alternating Nystagmus | Example of a patient with periodic alternating nystagmus, showing an alternation between left-beats and right-beats as the patient maintains forward gaze. Nystagmus maintain horizontal direction regardless of position of gaze. | Image/MovingImage |
| 141 |
 |
Physiologic (End-Gaze) Nystagmus | Demonstration of physiological nystagmus, where oscillations do not represent pathology, but occur when the patient's gaze is drawn too far laterally. | Image/MovingImage |
| 142 |
 |
Progressive Supranuclear Palsy | Progressive Supranuclear Palsy | Image/MovingImage |
| 143 |
|
Progressive Supranuclear Palsy | Example of patient with progressive supranuclear palsy. Discussion of difference between saccadic movement in supranuclear palsy and nystagmus. Shows saccadic intrusions in forward gaze, pursuit, saccades, and doll's head maneuver. | Image/MovingImage |
| 144 |
 |
Pulsating Exophthalmos | Example of a patient with neurofibromatosis with an absent sphenoid wing. Shows left eye pulsating back and forth with the pulse from front and side views. | Image/MovingImage |
| 145 |
 |
Pupil Signs in a 32-year-old Woman with Right-sided Adie's Pupil | Pupil signs in a 32-year-old woman with right-sided Adie's pupil. The right pupil is larger than the left pupil (top), reacts poorly to direct light stimulation (second panel), and better in response to near stimulation (third panel). The right pupil also shows a supersensitive response 30 minutes a... | Image |
| 146 |
 |
Pupillogram Demonstrating Paradoxical Pupillary Constriction to Darkness | Pupillogram demonstrating paradoxical pupillary constriction to darkness in four patients with congenital achromatopsia. Note that the pupils initially constrict when the light is extinguished. (Price MJ, Thompson HS, Judisch GF et al: Pupillary constriction to darkness. Br J Ophthalmol 1981;69:205-... | Image |
| 147 |
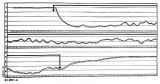 |
Pupillogram of a Healthy Young Subject | Pupillogram of a healthy young subject showing continuous pupillary oscillations of both pupils when light is sustained, indicated by the dark arrow at the top of the recording. Note that the oscillations of the pupils are synchronous and demonstrate variable amplitude and frequency. This pattern of... | Image |
| 148 |
 |
RAPD Present | This clip demonstrates the technique used to determine that Relative Afferent Pupillary Defect (RAPD) is present in a patient. | Image/MovingImage |
| 149 |
|
Rebound Nystagmus | Example of a patient with rebound nystagmus, where the oscillations alternate direction as the patient shifts gaze in different directions. Discussion of relationship to disease and disorders of the cerebellum, including degenerations of the cerebellum, infarction, and demyelination. | Image/MovingImage |
| 150 |
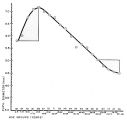 |
Relationship Between Age and Pupil Size | Relationship between age and pupil size, determined using an infrared flash photograph technique with subjects placed in darkness for 3 minutes. The numbers above the abscissa indicate the number of subjects tested in each age range. (Reprinted with permission of Loewenfeld IE: "Simple, central" ani... | Image |
| 151 |
 |
Retinal Fluorescein Angiography | This slide set provides a brief description of Retinal Fluorescein Angiography. First introduced in 1960, sodium fluorescein, a dye, is administered through an angiocatheter (3-5cc) by a nurse or technician. The dye reaches the central retinal artery after passing through the heart and lungs. | Text |
| 152 |
 |
Retinitis Pigmentosa Disease of Rods | Discussion of retinitis pigmentosa which is a retinal/choroidal degeneration caused by various genetic defects. | Text |
| 153 |
 |
Retino-choroidal Vessels or Optociliary Veins or Ciliary Shunt | Overview of retino-choroidal collaterals, which are potential telangiectatic connections between the retina and choroidal circulation. Although sometimes called "shunts", these collaterals are between the retinal venous circulation and the choroidal venous circulation. | Text |
| 154 |
 |
Retraction Nystagmus | Patient with retraction nystagmus (no audio) | Image/MovingImage |
| 155 |
 |
Right-sided Pseudo-Horner's Syndrome | Right-sided pseudo-Horner's syndrome in an 8-month-old infant referred because her mother had noted a larger pupil on the left for a few months and her pediatrician thought the right upper lid was droopy. Both pupils reacted normally to light and darkness, the degree of anisocoria was similar in bot... | Image |
| 156 |
 |
Right-sided Relative Afferent Pupillary Defect | Right-sided relative afferent pupillary defect in a man with optic nerve glioma. When the unaffected left eye is stimulated by light, both pupils constrict (top). When the light is then swung over to the affected right eye, both pupils dilate (bottom). This indicates that pupillomotor conduction thr... | Image |
| 157 |
 |
Rotary Downbeat | Patient with rotary downbeat nystagmus (no audio) | Image/MovingImage |
| 158 |
|
Rotary Nystagmus | Example of a patient with rotary nystagmus, showing occasional counterclockwise rotary movements of both eyes. Seen more in intrinsic disorders of the brainstem. | Image/MovingImage |
| 159 |
 |
Sector Palsies and Light-Near Dissociation | Example of patient with bilateral Adie's pupils. Exam is performed with a slit-lamp. Shows iris stroma and focal segments of iris sphincter that retain their contractilty. Suggests post-ganglionic parasympathetic denervation. | Image/MovingImage |
| 160 |
 |
See-saw Nystagmus | Example of a patient with see-saw nystagmus, showing how one eye elevates as the other depresses, with the elevating eye intorting as the depressing eye extorts. Shows vertical oscillations with pendular waveforms. Suggests a large structural lesion in the pericellar region (associated with bi-tempo... | Image/MovingImage |
| 161 |
 |
See-saw Nystagmus | 7-year-old female whose mother noticed her eyes "bouncing" for 2 months. Visual acuity 20/70 OD and 20/40 OS, reduced color vision OU, and no afferent pupillary defect. See-saw nystagmus documented with videography. Manual perimetry revealed a complete right homonymous hemianopia. MRI revealed a lar... | Image/MovingImage |
| 162 |
 |
See-saw Nystagmus MRI 1 | MRI; See-saw Nystagmus | Image |
| 163 |
 |
See-saw Nystagmus MRI 2 | MRI; See-saw Nystagmus | Image |
| 164 |
 |
Shaken Baby Syndrome | Text | |
| 165 |
 |
Shunt Vessel Meningioma | RETINO-CHOROIDAL (OPTO-CILIARY) COLLATERAL VESSELS: (also known as Retinal-choroidal venous collaterals, opticociliary veins or ciliary shunt vessels) Retino-choroidal collaterals are potential telangiectatic connections between the retina and choroidal circulation. Although sometimes called "shunts... | Image |
| 166 |
 |
Shunt Vessel Meningioma - MRI | Meningiomas block venous egress and open potential venous channels known as retinochoroidal (optociliary) collateral vein. This meningioma extends from the back of the globe through the optic canal. | Image |
| 167 |
 |
Spasm of the Near Reflex | Example of patient with spasm of the near reflex and voluntary nystagmus. Discussion of similar-looking conditions (e.g. six nerve palsy, limitation of abduction, lateral rectus muscle problems) and how to tell them apart from spasm of the near reflex by observing the myosis evoked by the near respo... | Image/MovingImage |
| 168 |
 |
Spasmus Nutans | Example of patient with spasmus nutans. Discussion of characteristics of this disorder, such as dissociated or monocular nystagmus, abnormal head position, and to-and-fro head oscillation. Sometimes an eccentric gaze is seen as well (as in patient). Patient has a monocular horizontal nystagmus in th... | Image/MovingImage |
| 169 |
 |
Spasmus Nutans | Example of patient with spasmus nutans. | Image/MovingImage |
| 170 |
 |
Spontaneous Venous Pulsations | This clips shows a spontaneous venous pulsation viewed during an ocular examination. | Image/MovingImage |
| 171 |
|
Square Wave Jerks | Example of patient with square wave jerks. Discussion of difference between square wave jerks (saccadic oscillations) and horizontal nystagmus. | Image/MovingImage |
| 172 |
 |
Stage 2 - Papilledema | Image | |
| 173 |
 |
Stages of Papilledema | Text | |
| 174 |
 |
Stargardt's Disease | Discussion of Stargardt's disease, an inherited maculopathy which frequently presents with a loss of central vision. | Text |
| 175 |
 |
Structures of the iris | Structures of the iris. The a indicates the anterior border layer that terminates at the pigmentary ruff of the pupillary border (b). The c indicates the iris sphincter muscle, which is oriented circumferentially within the stroma and located deep to the anterior border layer; d indicates vessels th... | Image |
| 176 |
 |
Superior Oblique Myokymia | Close-up video of a patient with superior oblique myokymia (no audio.) | Image/MovingImage |
| 177 |
 |
Superior Oblique Myokymia | Example of patients with superior oblique myokymia, a saccadic intrusion. First patient is seen to have intermittent, intorting movements with superimposed slight vertical deviations in right eye. Discussion of disorder as benign, but frequently disabling, as patients experience episodes of diplopia... | Image/MovingImage |
| 178 |
 |
Tadpole-shaped Pupil | Tadpole-shaped pupil in a 20-year-old women with frequent episodes of blurred vision and achiness of the right eye lasting several minutes. The patient took a photograph of her eyes during an attack to document the peaked, segmental dilation of her right pupil (black arow). (Thompson HS, Zackon DH, ... | Image |
| 179 |
 |
Test Duane | ||
| 180 |
 |
Testing the Visual Fields | Demonstration of various methods of testing visual fields, including counting fingers, motion, and color of several objects. | Image/MovingImage |
| 181 |
 |
Third Nerve Palsy | Patient with third nerve palsy (no audio) | Image/MovingImage |
| 182 |
 |
Third Nerve Palsy, Pupil Involving | Example of patient with third nerve palsy. Left eye shows pupilary involvement. Left eye doesn't immediately duct, but abducts well, with impaired superduction. Secondary and primary deviations are demonstrated. Anisocoria is more prominent when light is on, showing a parasympathetic defect to the p... | Image/MovingImage |
| 183 |
 |
Tour of the Direct Ophthalmoscope | This clip describes the parts and operation of the ophthalmoscope as an ocular examination tool. Includes adjustment of aperture size and adjustment of lenses. | Image/MovingImage |
| 184 |
 |
Tour of the Fundus | This clip demonstrates the funduscopic examination technique. | Image/MovingImage |
| 185 |
|
Transillumination - Ciliary Body Neurofibromas | Example of transillumination on a patient with neurofibromatosis, but without Lisch nodules. Shows suspected neurofibromas in the ciliary body. | Image/MovingImage |
| 186 |
|
Transillumination - Lisch Nodules | Demonstration of transillumination of the Lisch nodules on a patient with neurofibromatosis. Shows how Lisch nodules that were not very visible in slit-lamp examination are better seen with transillumination, which may therefore be useful in detecting Lisch nodules earlier in children where they are... | Image/MovingImage |
| 187 |
|
Transillumination Ocular Melanoma | Video describing condition. | Image/MovingImage |
| 188 |
 |
Unilateral Blepharospasm | Example of patient with unilateral blepharospasm. | Image/MovingImage |
| 189 |
 |
Upbeat Nystagmus | Example of a patient with upbeat nystagmus. Shows vertical jerk nystagmus with fast phases in the up direction. Localizes to brain stem, and occurs with strokes, demyelination, and tumors. | Image/MovingImage |
| 190 |
 |
Vestibular Nystagmus | Example of patient with vestibular nystagmus. Patient is led through instructions for direction of gaze. Shown also with Frenzel goggles. | Image/MovingImage |
| 191 |
|
Vestibular Nystagmus | Discussion of vestibular nystagmus. Seen with peripheral disorders and central disorders, and in two varieties: spontaneous and positional. Horizontal jerk with small amplitude. | Image/MovingImage |
| 192 |
 |
Voluntary Nystagmus | Example of patient with voluntary nystagmus. Discussion of how a lack of uniform, patterned movement of the eyes along with associated lid movements suggests that activity is voluntary. | Image/MovingImage |
| 193 |
 |
Wall-Eyed Bilateral Internuclear Ophthalmoplegia (WEBINO) | Example of patient with horizontal binocular diplopia. Demonstration of exam, which shows alternating exotropia in cover test. As patient follows object, right eye does not pass the midline as the object moves to the left, while left eye go slightly past the midline, but does not abduct completely. ... | Image/MovingImage |
| 194 |
 |
Wall-Eyed Bilateral Internuclear Ophthalmoplegia (WEBINO) | Example of patient with Wall-Eyed Bilateral Internuclear Ophthalmoplegia. Patient is led through instructions for direction and distance of gaze. | Image/MovingImage |
| 195 |
 |
The Wall-Eyed Potato Farmer | Young man presenting with apparent episodic neurologic evants that initially was thought to be multiple sclerosis, but as time went on, he had progressive changes in his neurologic exam and in his imaging findings. Brain biopsy revealed Gliomatosis cerebri. Anatomy: Brain Stem; Pons; Midbrain. Patho... | |
| 196 |
 |
Why Don't You See Double? | This presentation was given at the Neurology Grand Rounds in Fall 2011 at the University of Utah. A number of Duane Syndrome cases are covered. Related video can be found in this collection at: Duane's Syndrome Type I: http://content.lib.utah.edu/u?/EHSL-Moran-Neuro-opth,130 Duane's Syndrome Type I... | Text |
1 - 200 of 196