| Identifier |
walsh_2021_s2_c3-slides |
| Title |
Oh My GAD!! Something Else? |
| Creator |
Olwen Murphy; Kemar Green; John Probasco; Daniel Gold |
| Affiliation |
(OM) (KG) (JP) (DG) Johns Hopkins University School of Medicine, Baltimore, Maryland |
| Subject |
Nystagmus; Autoimmune Diseases |
| History |
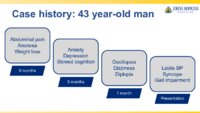
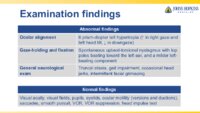
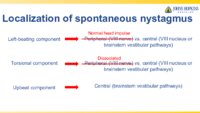
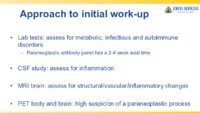
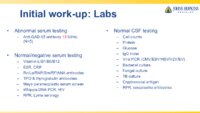
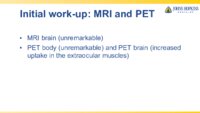
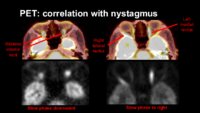
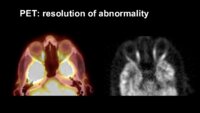
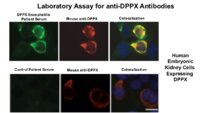
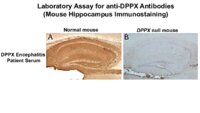
A 43 -year-old man presented with oscillopsia, dizziness, binocular vertical diplopia, and gait difficulties. He reported a six-month history of abdominal pain, anorexia and 50-pound weight loss, and a 3-month history of mood and cognitive changes. Torsional nystagmus, a left 4th nerve palsy (NP), unsteady gait, occasional head jerks, and intermittent facial grimacing were noted onexamination, and MRI brain/orbits was normal. Over weeks his symptoms worsened and he developed labile blood pressure and syncope. Repeat MRI, single-fiber EMG, myasthenic panel, celiac panel, TSH, cyanocobalamin, thiamine, RPR, copper, ESR, CRP, ANA, RF, ceruloplasmin, anti-ASO titers were normal. CSF and serum infectious, toxic, autoimmune and paraneoplastic panels were also within normal limits. He was referred to our institution 1 month after his initial assessment. Our evaluation demonstrated full ocular motility, a 6 prism-diopter left hypertropia (worse in right gaze and left head tilt, unchanged in upgaze and slightly less in downgaze), and spontaneous upbeat-torsional nystagmus with top poles beating toward the left ear and a milder left-beating component. Saccades, smooth pursuit, horizontal vestibulo-ocular reflex (VOR), VOR suppression and optokinetic nystagmus appeared unremarkable when taking into account the nystagmus. Afferent neuro-ophthalmic examination was normal. Serum anti-GAD antibody was positive (15 IU/mL, Normal <5.0 IU/mL). MRI brain and testicular ultrasound were normal. PET-CT showed increased FDG uptake in left medial rectus (MR), right lateral rectus (LR), and bilateral inferior recti (IR) muscles. Plasma exchange (PLEX) was initiated and his symptoms improved. Several days later, serum anti-dipeptidyl aminopeptidase-like protein 6 (DPPX) IgG returned as positive (titer 1:15.360), and the diagnosis of anti-DPPX-associated encephalitis was made. Screening for an underlying neoplasm was unrevealing, and treatment with rituximab was initiated. Nystagmus improved, and repeat PET-CT demonstrated resolution of the prior extraocular muscle (EOM) avidity. |
| Disease/Diagnosis |
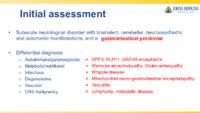
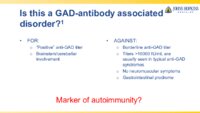
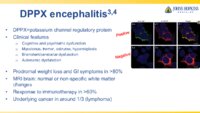
We considered paraneoplastic, autoimmune, infectious and nutritional etiologies in the differential diagnosis of this patient's subacute weight loss, neuropsychiatric symptoms, diplopia and nystagmus. The borderline positive GAD65-antibody (15 IU/mL) raised the possibility of an associated neurological syndrome, however typical anti-GAD-associated neurological syndromes are usually associated with high concentration serum anti-GAD antibodies (>10,000 IU/mL), while low concentration positivity is of uncertain clinical significance [4]. By contrast, anti-DPPX antibodies were identified at high concentration, and the prodromal gastrointestinal syndrome followed by encephalitis with prominent neuropsychiatric and brainstem involvement is highly characteristic for anti-DPPX antibody-associated encephalitis [5]. |
| Date |
2021-02 |
| References |
1. Jeong S, Oh Y, Kim C, Kim J. Bimedial rectus hypermetabolism in convergence spasm as observed on positron emission tomography. Journal of neuro-ophthalmology 2008;28:217-218. doi: 10.1097/WNO.0b013e3181772b02. 2. Ivanir Y, Trobe JD. Comparing hypertropia in upgaze and downgaze distinguishes congenital from acquired fourth nerve palsies. J Neuroophthalmol 2017;37:365-368. doi: 10.1097/WNO.0000000000000460. 3. Hernowo A, Eggenberger E. Skew deviation: Clinical updates for ophthalmologists. Curr Opin Ophthalmol 2014;25:485-487. doi: 10.1097/ICU.0000000000000105. 4. Muñoz-Lopetegi A, de Bruijn M, Boukhrissi S, et al. Neurologic syndromes related to anti-GAD65: Clinical and serologic response to treatment. Neurol Neuroimmunol Neuroinflamm 2020;7:e696. doi: 10.1212/NXI.0000000000000696. 5. Hara M, Ariño H, Petit-Pedrol M, et al. DPPX antibody-associated encephalitis: Main syndrome and antibody effects. Neurology 2017;88:1340-1348. doi: 10.1212/WNL.0000000000003796. |
| Language |
eng |
| Format |
application/pdf |
| Format Creation |
Microsoft PowerPoint |
| Type |
Text |
| Source |
53rd Annual Frank Walsh Society Meeting |
| Relation is Part of |
NANOS Annual Meeting Frank B. Walsh Sessions; 2021 |
| Collection |
Neuro-Ophthalmology Virtual Education Library: Walsh Session Annual Meeting Archives: https://novel.utah.edu/Walsh/ |
| Publisher |
North American Neuro-Ophthalmology Society |
| Holding Institution |
Spencer S. Eccles Health Sciences Library, University of Utah |
| Rights Management |
Copyright 2021. For further information regarding the rights to this collection, please visit: https://NOVEL.utah.edu/about/copyright |
| ARK |
ark:/87278/s6qk3g52 |
| Setname |
ehsl_novel_fbw |
| ID |
1694321 |
| Reference URL |
https://collections.lib.utah.edu/ark:/87278/s6qk3g52 |