A collection of videos relating to the diagnosis and treatment of eye movement disorders. This collection includes many demonstrations of examination techniques.
Dan Gold, D.O., Associate Professor of Neurology, Ophthalmology, Neurosurgery, Otolaryngology - Head & Neck Surgery, Emergency Medicine, and Medicine, The Johns Hopkins School of Medicine.
A collection of videos relating to the diagnosis and treatment of eye movement disorders.
NOVEL: https://novel.utah.edu/
TO
Filters: Collection: "ehsl_novel_gold"
| Title | Description | Type | ||
|---|---|---|---|---|
| 176 |
 |
Valsalva (Closed Glottis) | Valsalva (closed glottis or pinched nose): instruct the patient to take a deep breath and ‘bear down' (closed glottis) or take a deep breath and ‘try to pop their ears' (pinched nose). Assess for nystagmus. In superior canal dehiscence, pressure changes may be transmitted to the superior canal, ... | Image/MovingImage |
| 177 |
 |
Vibration | Vibration: instruct the patient to self-administer this test with an electric toothbrush or vibrator/massager, if available. Vibration of the mastoids and vertex will induce an ipsilesional slow phase with unilateral vestibular loss (https://collections.lib.utah.edu/details?id=1427582). | Image/MovingImage |
| 178 |
 |
VOR Suppression | VOR suppression (VORS): instruct the patient to fix on the camera which they should hold in front of their eyes, while turning their torso slowly in the horizontal plane. The vertical plane can then be assessed by instructing the patient to flex and extend the neck under the same conditions. A demon... | Image/MovingImage |
| 179 |
 |
Test Your Knowledge - The Acute Vestibular Syndrome and Ptosis | What is the most likely localization in this patient presenting with vertical diplopia and acute onset prolonged vertigo? A. Right medial longitudinal fasciculus (MLF) B. Left medial longitudinal fasciculus C. Right medulla D. Left medulla E. Left midbrain A. Incorrect. A right MLF lesion (stroke, M... | Image/MovingImage |
| 180 |
 |
The Bedside Examination of the Ocular Motor System | A masterclass covering the bedside examination of the ocular motor system. | Image/MovingImage |
| 181 |
 |
Central HINTS (With an Abnormal Head Impulse Sign) in the Acute Vestibular Syndrome Due to Lateral Pontine/Middle Cerebellar Peduncle Demyelination | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 30-year-old man presenting with vertigo, diplopia and mild left facial weakness (not seen in the video). On exam, there was right-beating nystagmus (RBN) in primary gaze that increased in right gaze (in accordan... | Image/MovingImage |
| 182 |
 |
HINTS Exam and Saccadic Dysmetria in Lateral Medullary Stroke | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a 50-year-old who experienced the abrupt onset of prolonged vertigo following chiropractic therapy 2 months prior. Initial work-up included an MRI and MR angiogram - MR-diffusion weighted imaging showed an acute l... | Image/MovingImage |
| 183 |
 |
Multiple Cranial Neuropathies Due to Glomus Tumor | This is a woman who was diagnosed with a right sided glomus tumor, and subsequently underwent resection. Seen here are multiple cranial neuropathies related to the tumor itself as well as to the surgery. She cannot abduct the right eye due to a right CN VI palsy. She has a right lower motor neuron f... | Image/MovingImage |
| 184 |
 |
Multiple Lower Cranial Neuropathies Following Carotid Endarterectomy | This is a patient who underwent a right carotid endarterectomy (CEA). Following the surgery, multiple right sided lower cranial nerves were involved. In his case, there was trapezius and sternocleidomastoid weakness and atrophy on the right, indicative of right CN XI injury. There was an absent gag ... | Image/MovingImage |
| 185 |
 |
Oculogyric Crisis | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This is a patient with neuroleptic-induced oculogyric crisis. 𝗡𝗲𝘂𝗿𝗼-𝗼𝗽𝗵𝘁𝗵𝗮𝗹𝗺𝗼𝗹𝗼𝗴𝘆 𝗮𝗻𝗱 𝗡𝗲𝘂𝗿𝗼-𝗼𝘁𝗼𝗹𝗼𝗴𝘆 𝗧𝗲𝘅𝘁𝗯�... | Image/MovingImage |
| 186 |
 |
Trigeminal Neuropathy with Loss of the Corneal Reflex | This is a woman who underwent radiofrequency ablation for left trigeminal neuralgia. Examination demonstrated loss of facial sensation on the left in addition to an absent corneal reflex on the left, consistent with involvement of the V1 (ophthalmic) branch of the trigeminal nerve. When the cornea i... | Image/MovingImage |
| 187 |
 |
The Virtual (Telemedicine) Ocular Motor Examination | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This document is based on Approach to the Ocular Motor & Vestibular History and Examination: https://collections.lib.utah.edu/ark:/87278/s64x9bq1, but adapted and edited for the telemedicine exam. Virtual Ocular Motor Ex... | Image/MovingImage |
| 188 |
 |
The Virtual (Telemedicine) Vestibular Examination | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: This document is based on Approach to the Ocular Motor & Vestibular History and Examination: https://collections.lib.utah.edu/ark:/87278/s64x9bq1, but adapted and edited for the telemedicine exam. Virtual vestibular ex... | Image/MovingImage |
| 189 |
 |
Audiometry | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: Audiometry is the measurement of the sensitivity and range of an individual's hearing. As many etiologies of imbalance, nystagmus, vertigo and/or dizziness can have an otologic origin the audiogram is an important piece o... | Text |
| 190 |
 |
Rotary Chair Testing | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: Rotary chair testing includes rotation around a vertical axis, and evaluates the horizontal semicircular canal vestibulo-ocular reflex (VOR). The patient sits in a mechanized chair with the head secured in a neutral posi... | Text |
| 191 |
 |
Evaluation of Auditory Function Using Rinne and Weber Tests | 𝗢𝗿𝗶𝗴𝗶𝗻𝗮𝗹 𝗗𝗲𝘀𝗰𝗿𝗶𝗽𝘁𝗶𝗼𝗻: The Rinne test is an assessment of auditory thresholds to air and bone conduction of sound. The Weber test is a comparison of bone conducted sound of either ear. Conductive hearing loss results in a loss of air conducte... | Image/MovingImage |
| 192 |
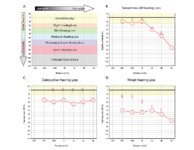 |
Audiometry: What Does It Look Like and How Do I Interpret It? | An audiogram measures a patient's auditory threshold responses with pure-tone stimuli across a range of sound frequencies that are important for human communication, typically 250 Hz to 8000 Hz. The threshold is the sound intensity level at which an individual detects the tone 50% of the time. Heari... | Text |
| 193 |
 |
What is the Cause of My Patient's Hearing Loss? | This is a flowsheet differentiating multiple causes of hearing loss. The onset and chronicity of hearing loss is a critical starting point in understanding whether urgent action is needed, such as in the setting of suspected stroke or sudden sensorineural hearing loss. For hearing loss that has been... | Text |
| 194 |
 |
The Affected-Ear-up 90 degree Maneuver (HC-Canalithiasis) | The Affected-Ear-up 90 degree Maneuver is used to treat horizontal canal-canalithaisis. 1. The patient starts in a supine position. 2. The patient rotates their head 90 degrees towards the unaffected side. 3. The patient sits up. | Text |
| 195 |
 |
The Affected-Ear-up 90 degree Maneuver (HC-Canalithiasis) (Video) | The Affected-Ear-up 90 degree Maneuver is used to treat horizontal canal-canalithaisis. 1. The patient starts in a supine position. 2. The patient rotates their head 90 degrees towards the unaffected side. 3. The patient sits up. | Image/MovingImage |
| 196 |
 |
Bow and Lean Test | The Bow and Lean Test is used to identify the affected side and is designed to be used in conjunction with or after the Supine Roll Test. Within this test a null point may exist where the nystagmus will extinguish because the cupula is in a gravity neutral position. As this test involves the patient... | Text |
| 197 |
 |
Bow and Lean Test (Video) | The Bow and Lean Test is used to identify the affected side and is designed to be used in conjunction with or after the Supine Roll Test. Within this test a null point may exist where the nystagmus will extinguish because the cupula is in a gravity neutral position. As this test involves the patient... | Image/MovingImage |
| 198 |
 |
The Canalith Repositioning Maneuver/Epley Maneuver for Right Posterior Canal Benign Paroxysmal Positional Vertigo | Posterior canal (PC) accounts for 70-90% cases of BPPV [1-3] and resolves with canalith repositioning maneuvers 90% of the time [4-20]. The Epley maneuver is considered a gold-standard treatment, with class 1 evidence for use. | Text |
| 199 |
 |
The Canalith Repositioning Maneuver/Epley Maneuver for Right Posterior Canal Benign Paroxysmal Positional Vertigo (Video) | Posterior canal (PC) accounts for 70-90% cases of BPPV [1-3] and resolves with canalith repositioning maneuvers 90% of the time [4-20]. The Epley maneuver is considered a gold-standard treatment, with class 1 evidence for use. | Image/MovingImage |
| 200 |
 |
The Gans Maneuver for Right Posterior Canal Benign Paroxysmal Positional Vertigo | This maneuver is recommended for individuals with cervical restrictions or precautions, as the maneuver avoids cervical hyperextension and may reduce cervical pain associated with repositioning maneuvers. The Epley maneuver has higher subjective and objective success rates compared to the Gans maneu... | Text |